Introduction
The SARS-CoV-2 pandemic and recent economic inflation has disproportionately impacted underserved and marginalized communities already facing low financial resources.1,2 Chronic conditions, such as diabetes, were diagnosed more after having COVID.3,4 Prevalence of obesity increased, likely due to less access to healthy foods and fewer opportunities for physical activity.3 Mental health conditions and substance use disorders were more prevalent.5
In response to COVID-19 related health disparities, the National Institutes of Health launched the national Community Engagement ALliance (CEAL) in fall 2020. The initial emphasis of CEAL was to address COVID-19–related inequities through community-engaged strategies to build trust, address health misinformation, and collaboratively address emerging health concerns. As the acute public health emergency subsided, the South-Central Texas CEAL, in alignment with the national CEAL, expanded its scope to chronic diseases and other pressing health needs in the post-pandemic period.
The objective of this study was to 1) assess the prevalence of chronic diseases at the community level, 2) identify barriers that community members face in accessing medical care, and 3) understand the socioeconomic resources needed during the post-COVID-19 pandemic period in Bexar County, TX and surrounding rural areas.
Methods
The South-Central Texas CEAL research team at UT Health San Antonio Department of Family and Community Medicine partnered with 17 established and trusted community and health-based organizations based in Bexar, Frio, Karnes, and Atascosa Counties. The partner organizations included nonprofits, South Central Area Health Education Center, the local health authority, Translational Advisory Boards, Alamo Colleges, rural hospital systems, and rural community health centers. (See Table 1) This report focuses on year 3 of the South-Central Texas CEAL initiative.
The annual “Common Survey” was developed by the NIH for all CEAL sites. The survey was designed to engage vulnerable communities and explore their attitudes and perceptions related to COVID-19, as well as assess the prevalence of chronic disease, social determinants of health, vaccine uptake, sources of health information, and trust. The South-Central Texas CEAL partners contributed to these surveys by adding questions based on local concerns. They distributed the surveys to their communities, using the results to inform outreach activities and apply for grants to address health disparities. The CEAL year 3 Common survey was distributed from March 2024 to July 2024.
The survey was written at a 7th grade reading level and translated into Spanish. One organization providing refugee services administered the survey to Afghan refugees using an interpreter. Surveys were distributed through an email link or completed on paper.
Eligible participants were adults aged 18 years and older who could understand and complete the survey. Community members under age 18 and individuals with cognitive impairments that would prevent comprehension of the survey were excluded.
The study protocol was reviewed and approved by the Institutional Review Board at UT Health San Antonio. Descriptive statistics were used to analyze the data, focusing on demographic characteristics, chronic disease prevalence, barriers to healthcare, and social determinants of health.
Results
A total of 685 community members completed the survey. The mean age of respondents was 45.9 years. The sample was predominantly male (74.2%) and three-quarters identified as Hispanic/Latino (75.2%). Household income was widely distributed, though over 19% of participants reported earning less than $25,000 annually, reflecting the economic vulnerability of the surveyed communities. See Table 2 for further demographic information.
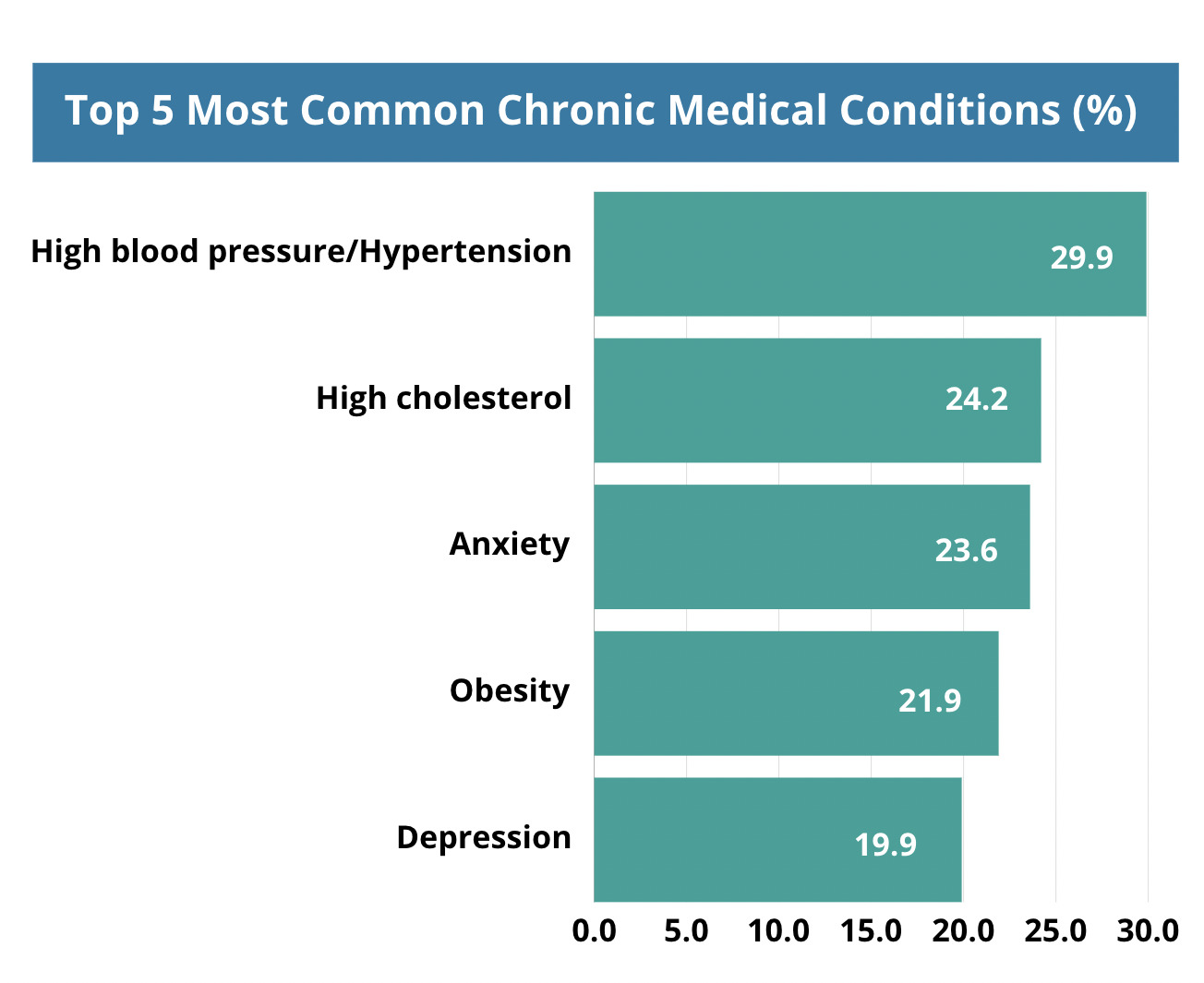
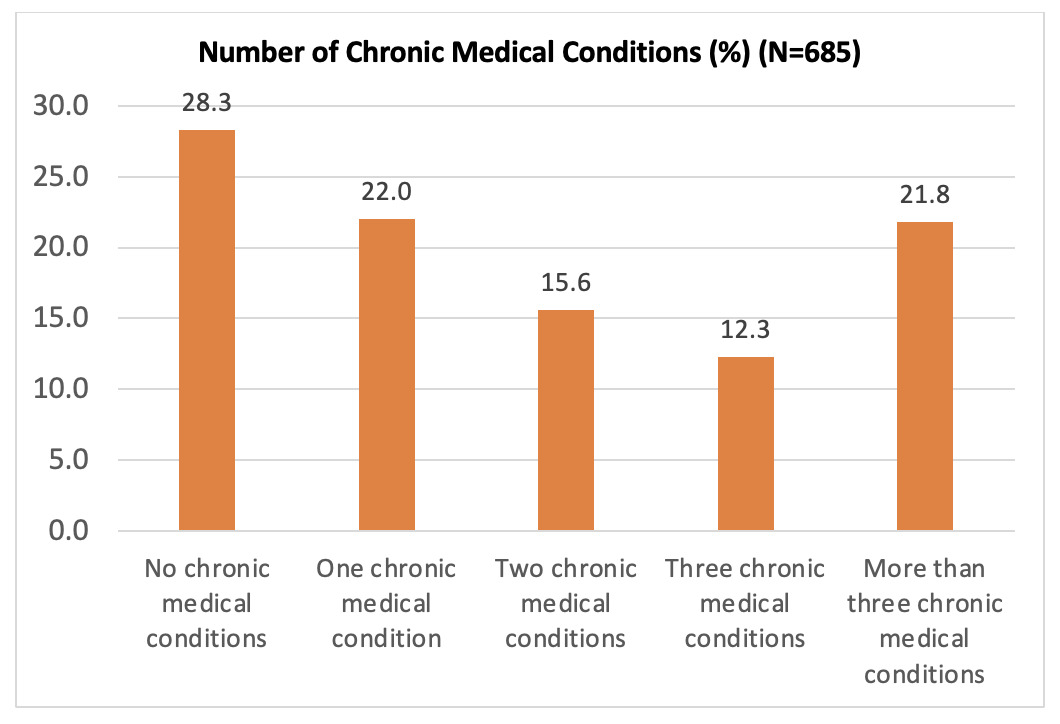
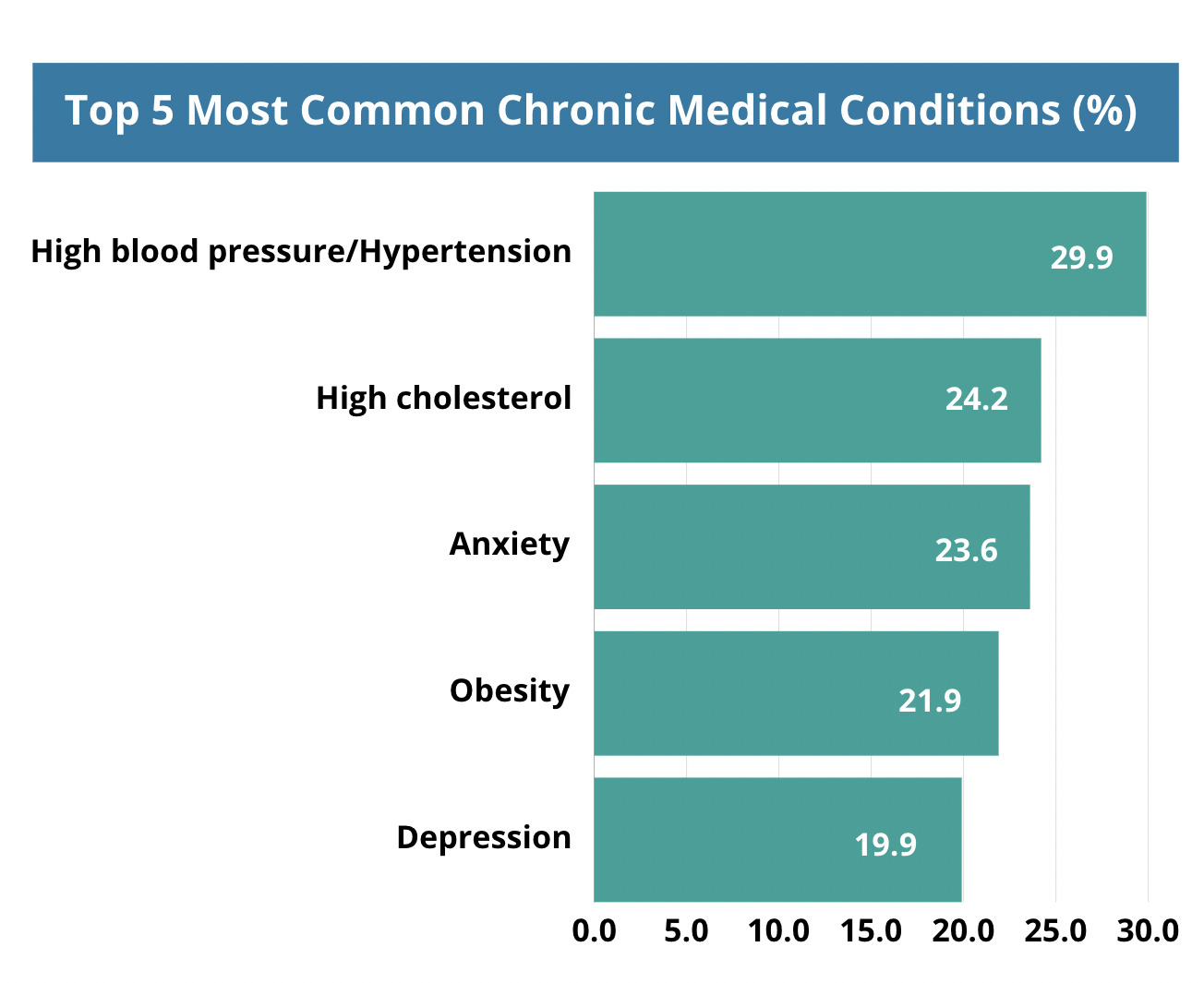
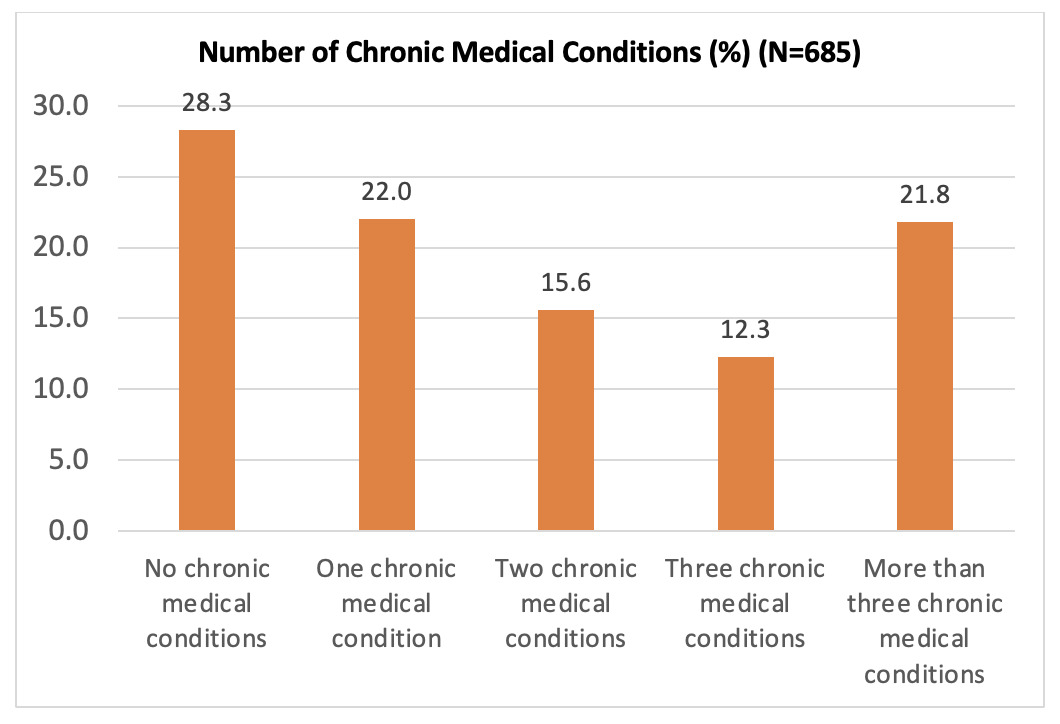
The prevalence of diabetes in the surveyed population was 16.5%. In addition to diabetes, respondents reported other chronic health conditions, with 21.8% reporting that they have more than three chronic conditions (Figures 1 and 2). Diabetes, hypertension, cardiovascular disease, cancer, and mental health/domestic violence were the top five conditions the communities wanted to learn more about.
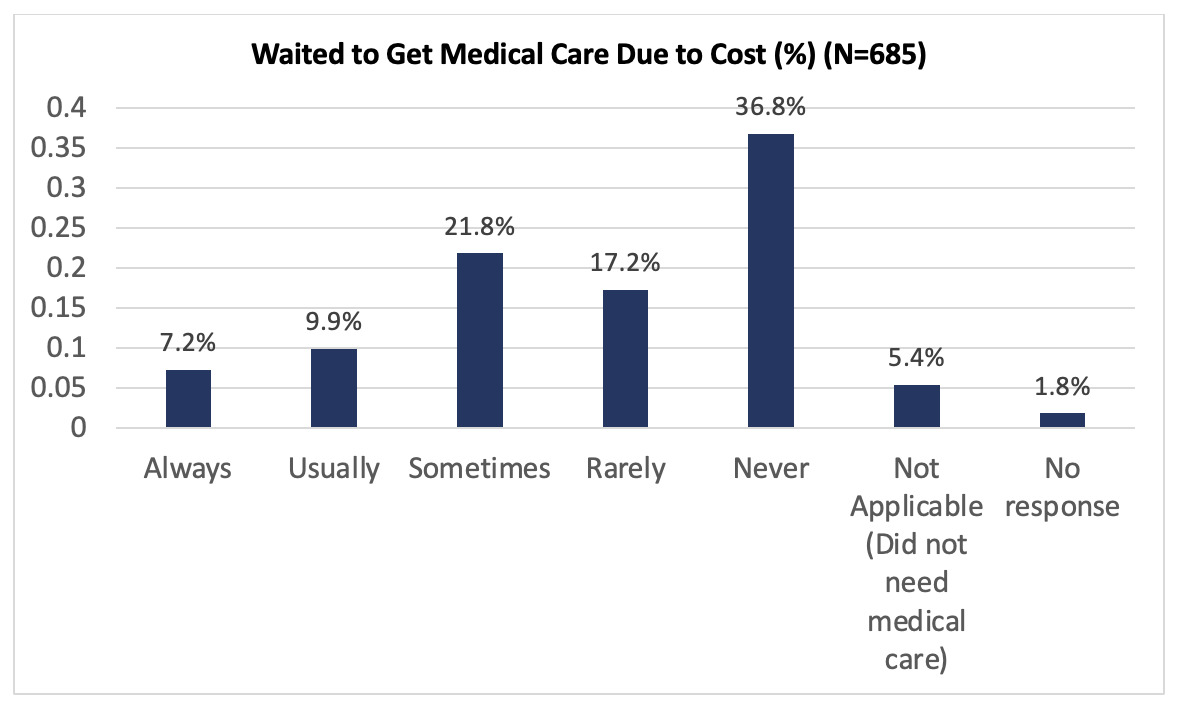
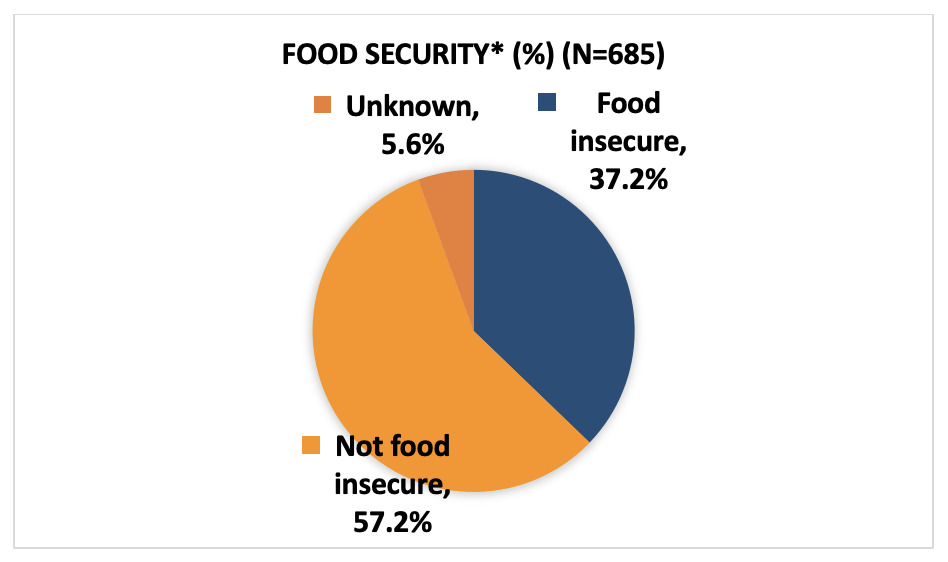
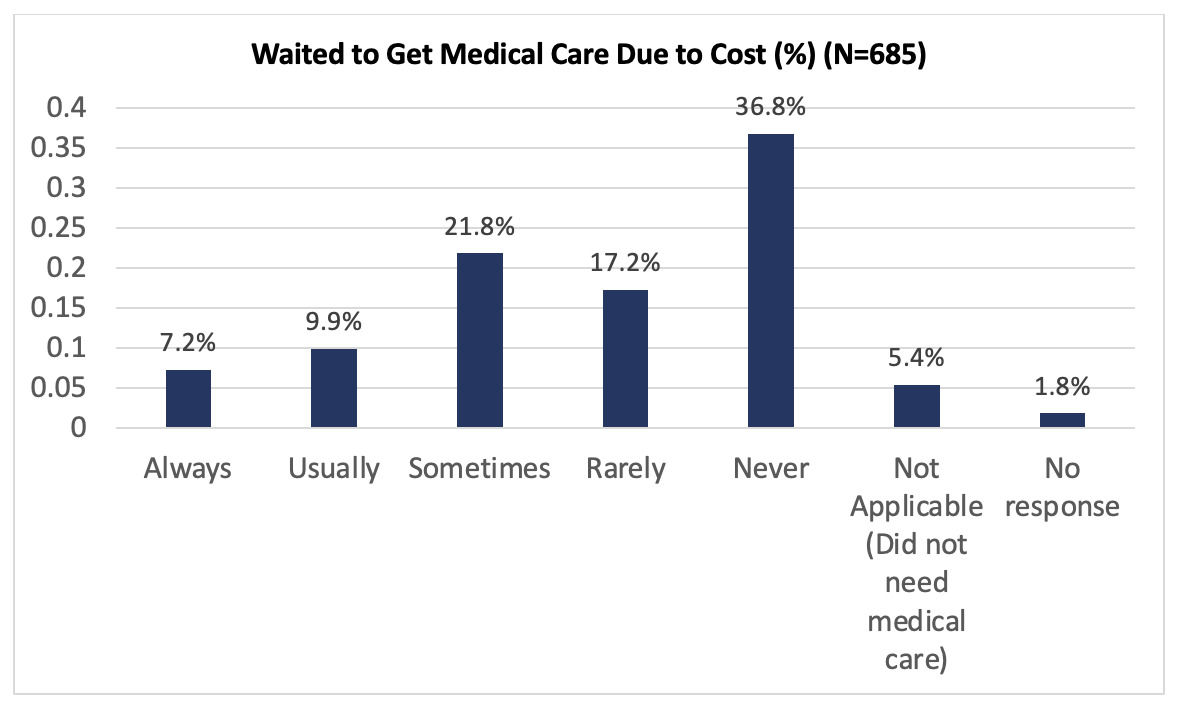
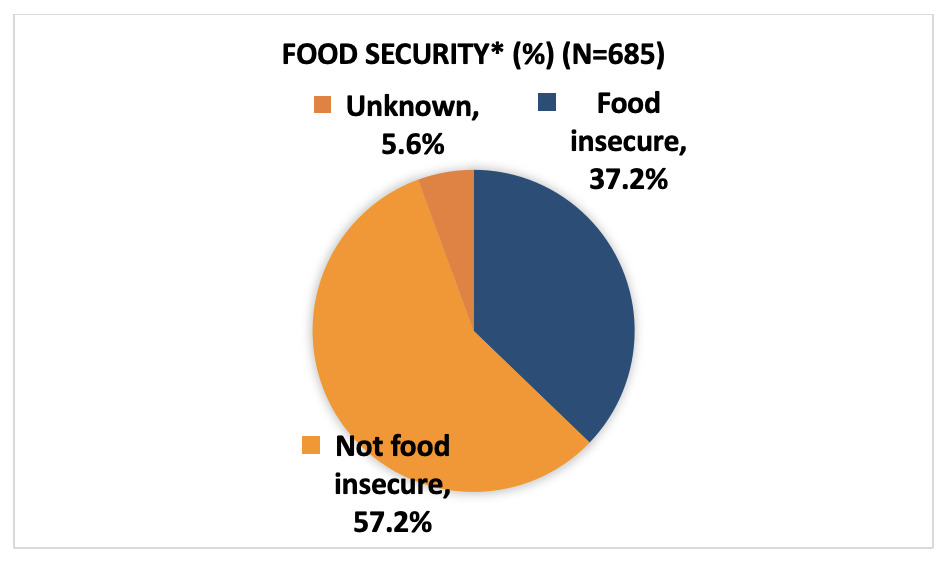
Significant barriers to care were also identified. More than a third of the respondents indicated that they at least sometimes delayed seeking medical care due to cost (Figure 3). Furthermore, 37.2% of participants had food insecurity based on the screening tool The Hunger Vital SignTM (Figure 4).6
Discussion
This study highlights the significant burden of multiple chronic diseases among underserved populations in South-Central Texas in the post-pandemic period. The prevalence of diabetes in the South-Central Texas CEAL partners’ communities was especially high at 16.5%. This rate is notably higher than the national average of 11.6%, Texas average of 12.3%, and Bexar County average of 13.2%.7,8 Since the South-Central Texas CEAL partners represent predominantly Hispanic/Latino, African American, immigrant, and rural Texas communities, these findings confirm long-standing concerns that these communities face disproportionate risk for diabetes.9,10 Our study shows that these same communities unfortunately also face significant barriers to timely medical care and encounter socioeconomic challenges such as food insecurity, which have been shown to negatively impact their ability to effectively manage their chronic conditions.11–13
The COVID-19 pandemic likely contributed to this heightened burden.1 National evidence demonstrates that SARS-CoV-2 infection is associated with increased risk of new diabetes diagnoses, particularly within the first month following infection.4 The pandemic also disrupted daily life in ways that exacerbated chronic disease risk.3 Job losses and economic instability reduced the ability of families to access healthy food or afford medical care, while the closure of schools, gyms, and community centers diminished opportunities for physical activity.
Social determinants of health—such as income, education, food access, and affordability of healthcare—continue to shape outcomes in vulnerable communities across South Central Texas. Addressing these inequities requires multifaceted approaches that extend beyond clinical care. Over the past three years, South-Central Texas CEAL partners have built trust with one another and with their communities, enabling collaboration that strengthens local capacity. These relationships can be used to facilitate resource-sharing, disseminate trusted health information, and connect community members to existing resources. Moreover, they position CEAL partners to collectively advocate for policy changes that address structural barriers and support vulnerable communities in managing their chronic conditions.
Conclusion
There is a substantial burden of chronic disease in Bexar County and surrounding rural counties. However, the communities face significant barriers to timely medical care and encounter socioeconomic challenges, which have been shown to negatively impact their ability to effectively manage their chronic conditions. Future South-Central Texas CEAL initiatives will build on the trust established with community partners to strengthen connections to health and social resources through resource sharing, educational messaging, and community engagement.