
INTRODUCTION
Among men aged 15-35 years, testicular cancer is one of the most common solid organ malignancies.1 In the United States, over 8,000 new cases are diagnosed annually, with a greater than 95% five-year survival rate when identified and treated early.1 Ultrasound is the first-line imaging modality used to evaluate testicular pathology and rule out non-malignant conditions such as torsion and hydrocele.1,2 Strong handheld ultrasound skills are essential for primary care physicians in low-resource settings, as they can provide immediate diagnostic information and enable timely escalation of care. This case highlights the role of point-of-care ultrasound in facilitating early diagnosis and escalation of care for testicular malignancy in a low-resource primary care setting.
CASE PRESENTATION
A 21-year-old male with no significant past medical history presented to a low-resource primary care clinic for routine health screening and laboratory evaluation. Initial laboratory work demonstrated microscopic hematuria with 11-30 red blood cells per high-power field (RBC/HPF). At the time of presentation, the patient denied dysuria, increased urinary frequency, or gross hematuria. Point-of-care renal ultrasound of the kidneys and bladder demonstrated no gross abnormalities; scrotal ultrasound was not performed at that time. The patient was referred to urology for further evaluation, where a CT urogram performed in July 2024 revealed no abnormalities of the kidneys, ureters, bladder, or urethra; incidental findings of left acetabular impingement were noted. He was advised to follow up in one year.
Several months later, repeat urinalysis in September 2024 again demonstrated microscopic hematuria, now with 1+ occult blood and 11-30 RBC/HPF. During follow-up evaluation, the patient continued to deny dysuria or gross hematuria. He endorsed increased urinary frequency but attributed this to increased daily water intake. However, the patient also reported left-sided scrotal swelling that began shortly after his prior urologic evaluation, accompanied by intermittent sharp pain in the left femoral region occurring every two to three days and rated as 4/10 in intensity. He denied progressive enlargement since onset, scrotal skin changes, systemic symptoms, or the presence of testicular lumps or nodules.
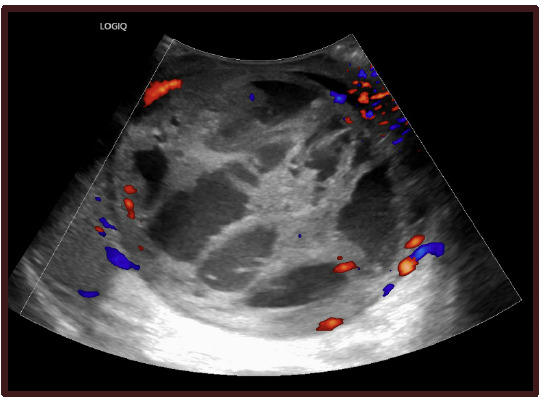
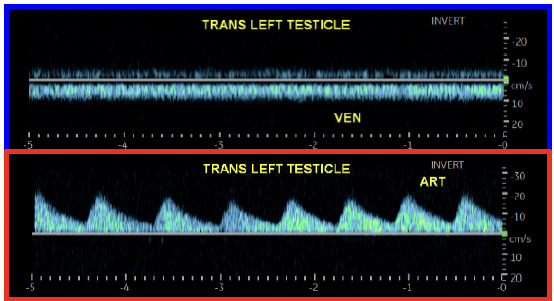
Physical examination revealed diffuse enlargement of the left hemiscrotum compared to the right, without overlying skin discoloration. Palpation of the left testicle demonstrated firmness without abnormal warmth, erythema, or tenderness. Given these findings, point-of-care scrotal ultrasound was performed, which demonstrated marked enlargement of the left testicle measuring approximately 9.0 x 10.0 cm compared to the contralateral right testicle measuring approximately 8.0 x 9.0 cm, without evidence of hydrocele or torsion. The left testicle demonstrated heterogeneous echogenicity with complex cystic areas and internal vascular septations (Figure 1). Duplex imaging further demonstrated preserved arterial and venous waveforms (Figure 2), helping exclude torsion and supporting intratesticular pathology.


The patient was advised to seek emergent evaluation, and subsequent imaging at the emergency department confirmed a 9.9 cm complex cystic mass with thick vascular septations replacing the left testicle, highly concerning for primary testicular malignancy. Serum tumor markers were elevated, including beta-human chorionic gonadotropin (β-hCG) at 39 IU/L (reference range: 0-3 IU/L) and alpha-fetoprotein (AFP) at 73.8 ng/mL (reference range: <6.1 ng/mL), and lactate dehydrogenase (LDH) at 284 U/L (reference range: 135–225 U/L) (Figure 3). Cross-sectional imaging demonstrated no evidence of metastatic disease in the chest, abdomen, or pelvis. The patient subsequently underwent left radical orchiectomy with testicular prosthesis insertion via a left inguinal incision in October 2024 without complication. Pathologic evaluation confirmed a mixed germ cell tumor measuring 9.8 x 8.0 x 7.0 cm, composed of teratoma (approximately 10%), embryonal carcinoma (approximately 85%), and yolk sac carcinoma (approximately 5%). Postoperative follow-up demonstrated appropriate surgical recovery. Staging workup revealed no evidence of metastatic disease, and the patient was referred to medical oncology for further evaluation and discussion of adjuvant management.
__beta-h.png)
DISCUSSION
Testicular cancer is the most common solid malignancy among men aged 15-35 years and is associated with excellent outcomes when diagnosed early.1 Typical presentations include painless testicular masses or scrotal swelling.1 However, atypical presentations such as hematuria are less common and may delay diagnosis.3 In this case, the patient initially presented with asymptomatic microscopic hematuria, which did not raise immediate concern for testicular malignancy and contributed to delayed recognition of the underlying disease.
Ultrasound remains the first line imaging modality for evaluation of scrotal pathology due to its accessibility, high sensitivity for detecting testicular tumors, and lack of ionizing radiation.1,2 In contrast, computed tomography urograms do not routinely include detailed evaluation of the scrotum or testicles and are not appropriate screening tools for testicular malignancy.2 The absence of abnormalities on the initial CT imaging likely contributed to the delay in diagnosis. Recognition of concerning sonographic features such as heterogeneous echogenicity, cystic components, and vascular septations is critical, as these findings necessitate urgent urologic referral.2
A normal testicle on ultrasound demonstrates homogeneous medium-level echogenicity with a smooth contour and symmetric size compared to the contralateral testis. In contrast, malignant intratesticular lesions typically appear as hypoechoic or heterogeneous masses with irregular borders, internal cystic changes, and increased internal vascularity on Doppler imaging. Importantly, solid intratesticular masses are considered malignant until proven otherwise.2 Early recognition of these sonographic characteristics in the primary care setting can significantly reduce delays in diagnosis and expedite definitive management.
Point-of-care ultrasound played a pivotal role in this case by enabling rapid identification of a concerning testicular mass in a low-resource primary care setting. Immediate visualization of abnormal findings facilitated prompt escalation of care and definitive surgical management. Primary care physicians are often the first point of contact for patients with sensitive genitourinary complaints, and proficiency in point-of-care ultrasound can significantly improve diagnostic efficiency in settings with limited access to advanced imaging.
Beyond individual case recognition, broader integration of point-of-care ultrasound into family medicine training is increasingly emphasized at both undergraduate and graduate medical education levels. A national survey of family medicine residency program directors found that 53% of programs report an established POCUS curriculum, with only 11% reporting no plans for implementation.4 Similarly, recent national data demonstrate that approximately 66% of U.S. allopathic medical schools have an approved POCUS curriculum, with most requiring ultrasound education during the preclinical years and an increasing number implementing longitudinal training models.5 These findings reflect substantial expansion and maturation of structured ultrasound education across medical training.6 Within Texas, academic institutions such as Texas Tech University Health Sciences Center have demonstrated successful integration of structured POCUS curricula within undergraduate medical education.7 This participation reflects regional engagement in ultrasound training within Texas medical education. Continued integration of structured POCUS curricula in Texas residency and medical school programs may further enhance early detection of serious pathology in primary care settings.
This case also highlights the importance of establishing patient rapport and maintaining a safe clinical environment. Sensitive genitourinary symptoms may not be disclosed immediately, which can contribute to delays in diagnosis. Open communication and trust between patients and clinicians may facilitate earlier symptom disclosure and improve timely identification of serious pathology.
CONCLUSION
This case demonstrates the utility of point-of-care ultrasound in identifying testicular malignancy and expediting escalation of care in a low-resource primary care setting. Recognition of concerning sonographic features allowed for timely urologic referral and definitive surgical management. As family medicine physicians are often the first point of contact for patients with genitourinary complaints, this case highlights the importance of maintaining open patient dialogue and recognizing atypical presentations. Strong ultrasound skills, combined with patient rapport, can significantly reduce diagnostic delays and improve clinical outcomes.