KEY POINTS
Question Does a brief educational intervention improve primary care clinicians’ awareness of firefighter occupational cancer risk?
Findings A thirty-minute educational lecture significantly improved clinician knowledge, with mean scores increasing from fifty percent to seventy percent.
Meaning Targeted, time-efficient education may enhance cancer prevention and screening for firefighters in family medicine settings and support compliance with the Wade Cannon Act, which requires Texas cities and municipalities to provide no-cost cancer screenings to firefighters beginning in the fifth year of employment and annually thereafter.
INTRODUCTION
Cancer is the leading cause of line-of-duty death (LODD) among firefighters, accounting for more than 75% of LODDs, according to the International Association of Fire Fighters (IAFF).1,2 LODD is defined as death resulting from a personal injury or illness sustained in the course of firefighting. However, existing cancer screening and prevention guidelines inadequately address the elevated occupational risk faced by this population.3
Firefighters are exposed to carcinogenic substances through multiple routes, including fires, diesel exhaust, contaminated protective equipment, and fire station environments. While fighting fires, they are exposed to more than 40 compounds designated carcinogenic by the International Agency for Research on Cancer (IARC), including asbestos, polycyclic aromatic hydrocarbons, benzene, hydrogen cyanide, formaldehyde, carbon monoxide, and polyfluoroalkyl substances (PFAs).4,5 These compounds could be ingested, inhaled, or absorbed by the skin. According to the CDC, these compounds have been known to increase the risk of cancers, as PFAs are able to activate oncogenes while inhibiting tumor suppressor genes.4,5 Other risk factors that could also contribute to increasing risk of cancers include lifestyle and shift-related factors such as sleep disruption, given that shift work has been classified as carcinogenic, as well as altered nutritional patterns.6,7
Family physicians and primary health care providers are often the first point of contact for firefighters seeking preventive care. Awareness of firefighter-specific cancer risks is therefore critical to improving early detection, counseling, and survivorship outcomes. This includes specific screening recommendations for cancers, such as skin, colorectal, and breast cancers. Other screening recommendations related to occupational health also include screening for hearing, pulmonary function, and mental health.8,9 However, limited formal education exists for clinicians regarding occupational cancer risk in the fire service.7,10
This quality improvement study was conducted to evaluate the impact of a targeted educational lecture on firefighter occupational cancer delivered to health care providers and assess their knowledge, attitudes, and behaviors using pre- and post-intervention questionnaires.
METHODS
Study Design
This quality improvement study employed a pre–post survey design to assess changes in health care provider knowledge and attitudes following an educational intervention.
Setting and Participants
The study was conducted at Health by Design, a primary care clinic serving retired police officers and firefighters in San Antonio, Texas. Participants included physicians, nurses, and clinical staff. A total of forty-six respondents completed the pre-intervention questionnaire and twenty-six completed the post questionnaire. Participation was voluntary and anonymous. There were no exclusion criteria.
Intervention
A company-wide, thirty-minute educational lecture titled Firefighters and Cancer: An Overview and Guide for Physicians and Healthcare Providers was delivered on July 24, 2025 by members of the research team. The lecture focused on occupational cancer risks associated with firefighting and strategies for early detection and prevention. The session began with an overview of occupational firefighter exposures and their classification as a known Group 1 human carcinogen by the International Agency for Research on Cancer (IARC).11,12 Participants were informed that cancer represents the leading cause of mortality among firefighters and that epidemiological data demonstrates a 9% increased risk of cancer incidence and a 14% increased risk of cancer-related mortality among firefighters compared with the general population, with emphasis that firefighters are not only affected by cancer at an earlier age, but may also be more susceptible to increased aggressiveness of these malignancies.2,3 The intervention reviewed the 21 types of cancers that affect firefighters and highlighted the mechanisms for occupational exposures primarily through inhalation, dermal absorption, and ingestion as alternative routes. Firefighters are at a significantly increased risk for at least 21 site-specific cancers, including malignancies of the bladder, brain and central nervous system (CNS), buccal cavity, pharynx, colon, Hodgkin lymphoma, non-Hodgkin lymphoma, kidney, leukemia, mesothelioma, multiple myeloma, pancreas, prostate, rectal, skin, stomach, testis, and thyroid.13,14
Although no singular cause for these cancers has been identified, the discussion broadly categorized the contributing risk factors. The modifiable and non-modifiable behavioral risk factors included inconsistent use of the self-contained breathing apparatus (SCBA), exposure to diesel exhaust, and cultural practices surrounding contaminated gear. In addition, sun exposure, poor nutrition, alcohol, tobacco use, obesity, and physical inactivity were associated with multiple malignancies. Additionally, sleep interruption due to shift and night work is categorized as Group 2A probable human carcinogens contributing to metabolic dysfunction, immune suppression, cardiovascular disease, and mental health concerns of firefighters.12,15
The intervention also included practical strategies to address the behavioral risk factors by placing a major emphasis on consistent use of SCBA and personal protective equipment. This is considered the single most important act firefighters can do to protect themselves from carcinogens, as well as utilizing proper decontamination practices associated with exposures from all phases of firefighting.16 For the environmental exposures, the talk recommended use of exhaust capture hoses to limit inhalation of diesel exhaust, HVAC separation systems for the engine bay and main station, and routine surface decontamination. Emphasis was placed on the use of sunscreen and other preventive lifestyle measures, including adoption of the mediterranean diet, physical activity, and maintenance of a healthy BMI. In addition, emphasis was also placed on counselling for alcohol and smoking cessation, promotion of sleep hygiene, and referral for a sleep study if there were any concerns.
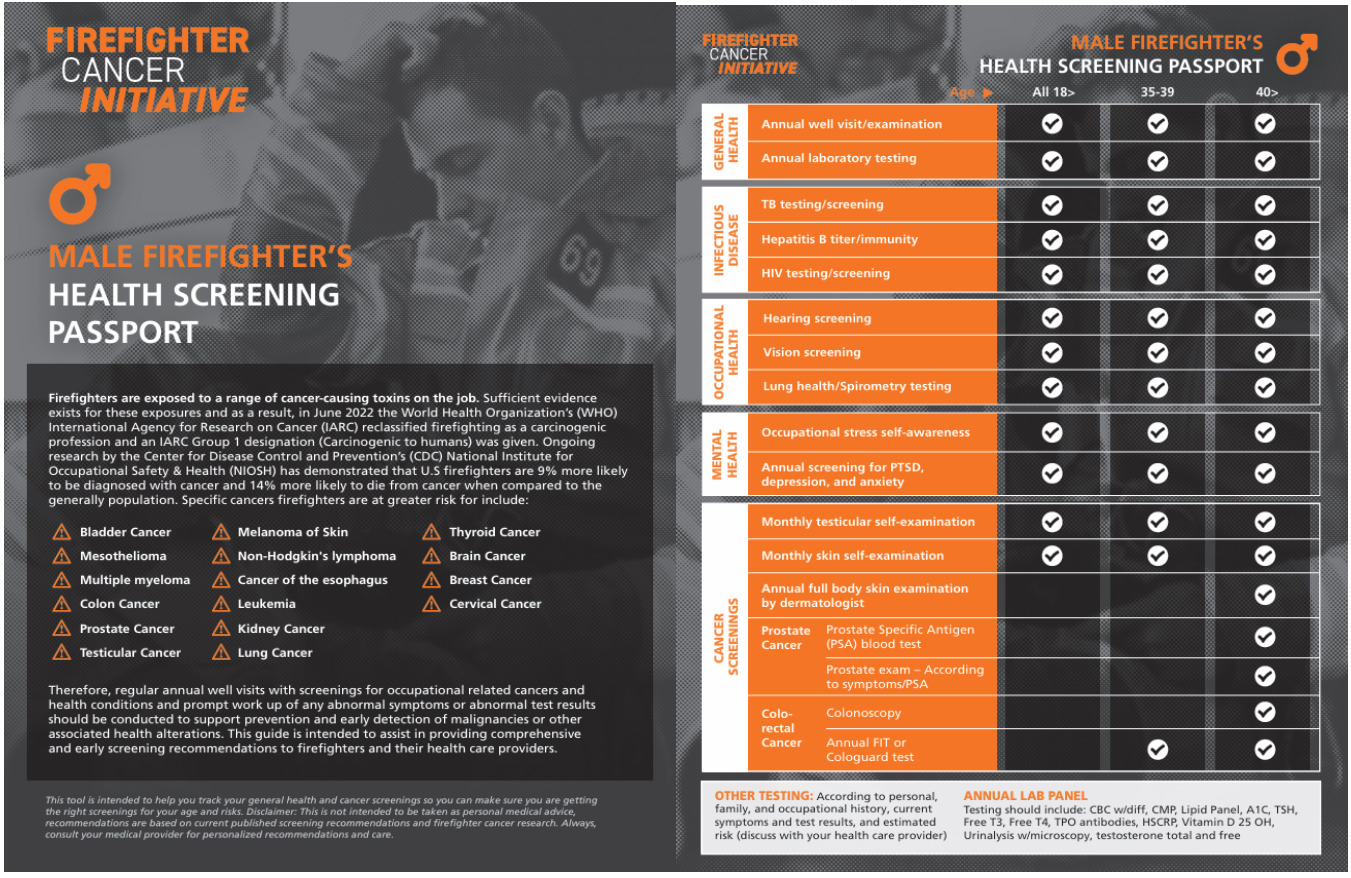
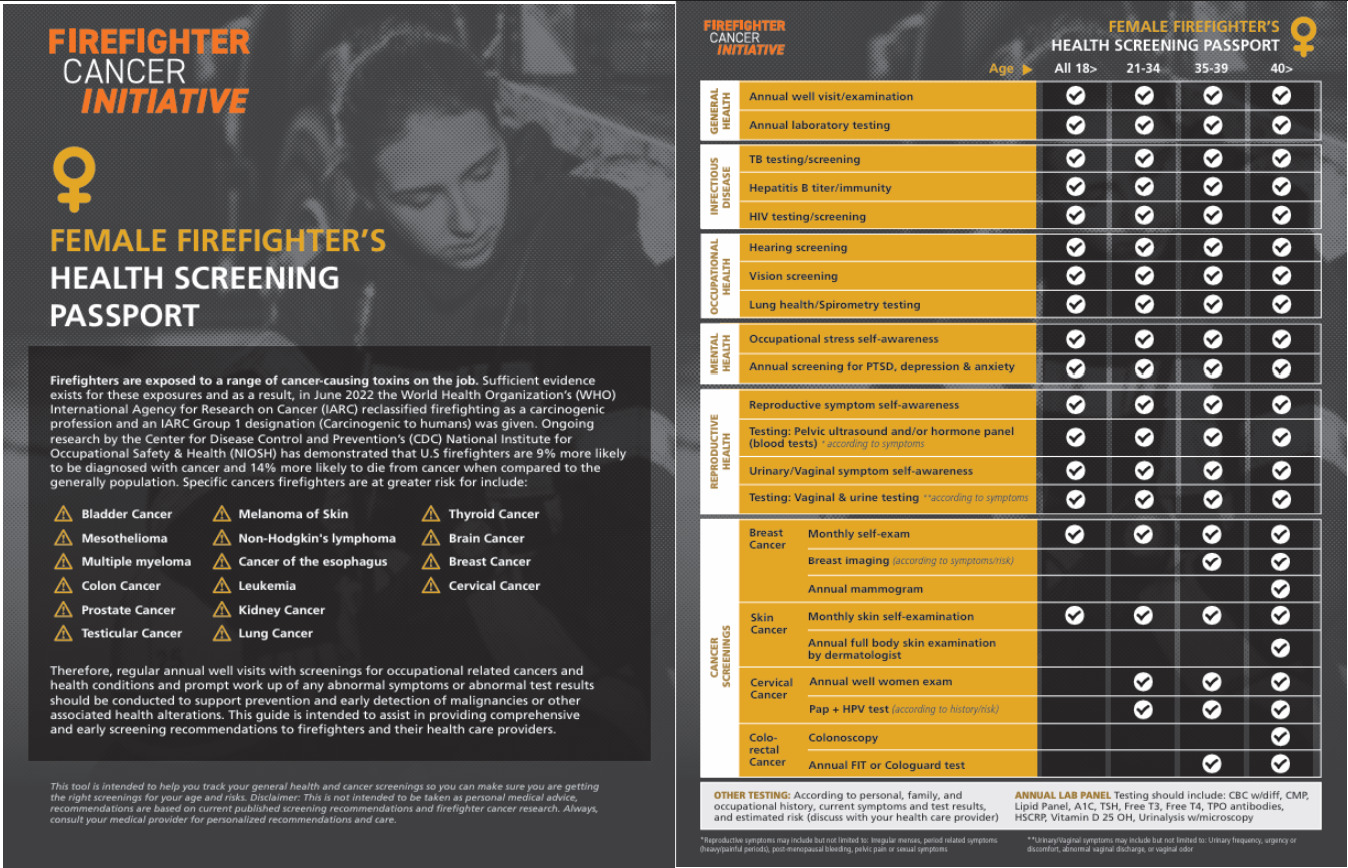
The lecture concluded with an overview of current initiatives aimed at reducing occupational cancer risk among firefighters. Participants were introduced to the Firefighter Health Screening Passport, which included recommendations for earlier initiation of dermatologic, colorectal, pulmonary, breast, and prostate cancer screening, as well as routine mental health monitoring.8 This passport was developed by the University of Miami and the Sylvester Cancer Center to support continuity of cancer prevention and screening recommendations for both male and female firefighters and health care providers. In partnership with the San Antonio Fire Department and UT Health San Antonio, these institutions have supported the implementation of firefighter-specific screening guidelines that cover information in addition to the USPSTF guidelines, including the need to screen for cancer earlier in firefighters.
Data Collection
Participants completed a voluntary questionnaire immediately before and after the intervention. Surveys assessed knowledge of firefighter occupational cancer risk, attitudes toward occupational screening, and perceived confidence in caring for firefighter patients. All responses were anonymized and blinded prior to analysis.
Outcomes
Primary outcomes included changes in overall knowledge scores. Secondary outcomes included item-level knowledge changes, Likert-scale measures of attitudes and behaviors, and post-intervention feedback.
Statistical Analysis
Pre- and post-intervention responses were compared using appropriate statistical tests via Excel. A two-sided p-value of less than 0.05 was considered statistically significant. Ninety-five percent confidence intervals were calculated where applicable.
Ethical Considerations
This project was conducted as a quality improvement initiative and did not involve patient-level data.
RESULTS
Participants
A total of forty-six health care providers completed the pre-intervention questionnaire, and twenty-six completed the post-intervention questionnaire. All surveys were voluntary and anonymous.
Knowledge Outcomes
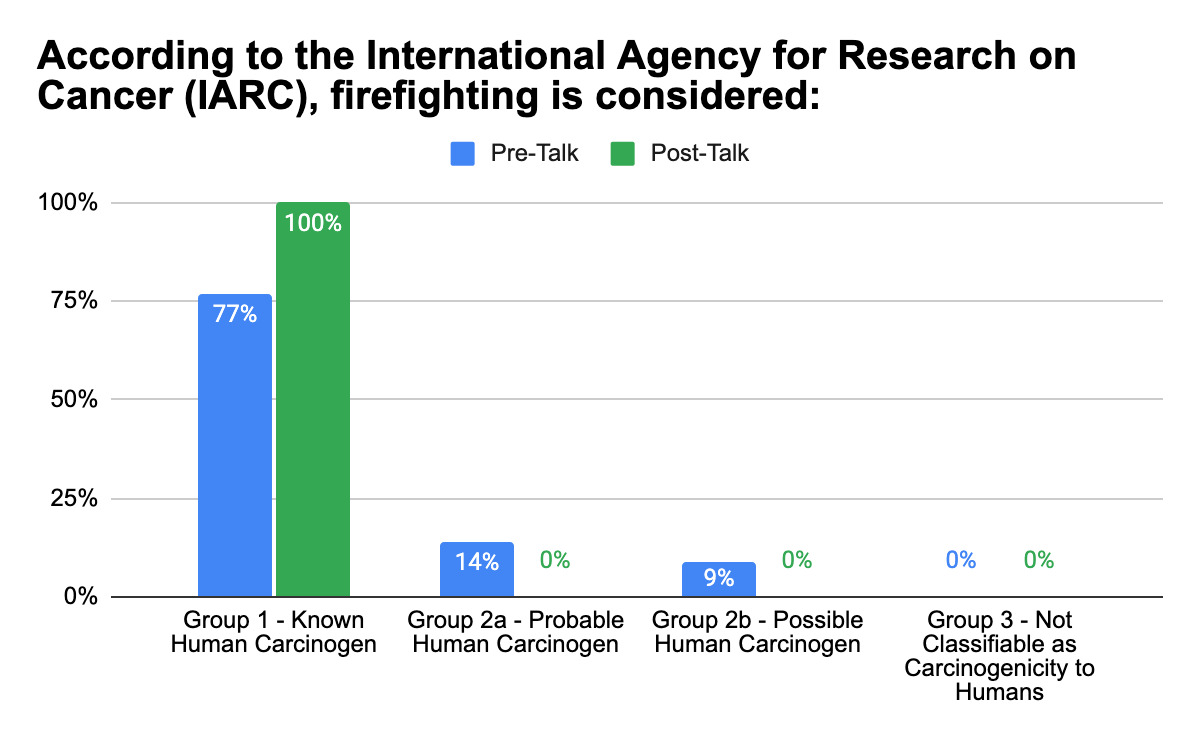
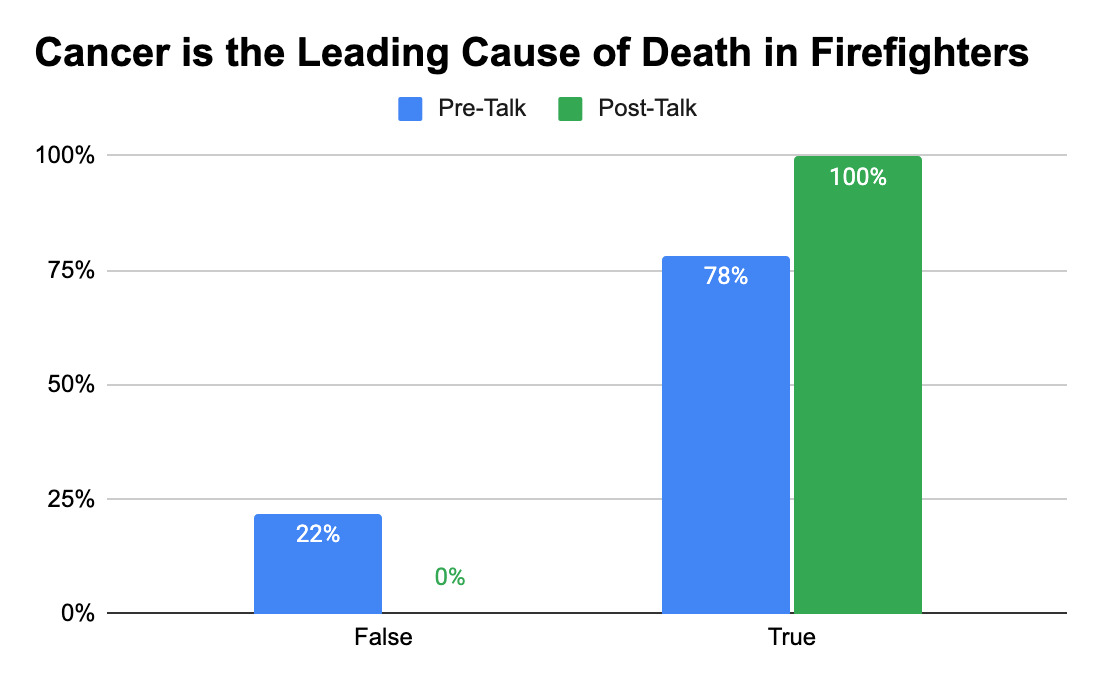
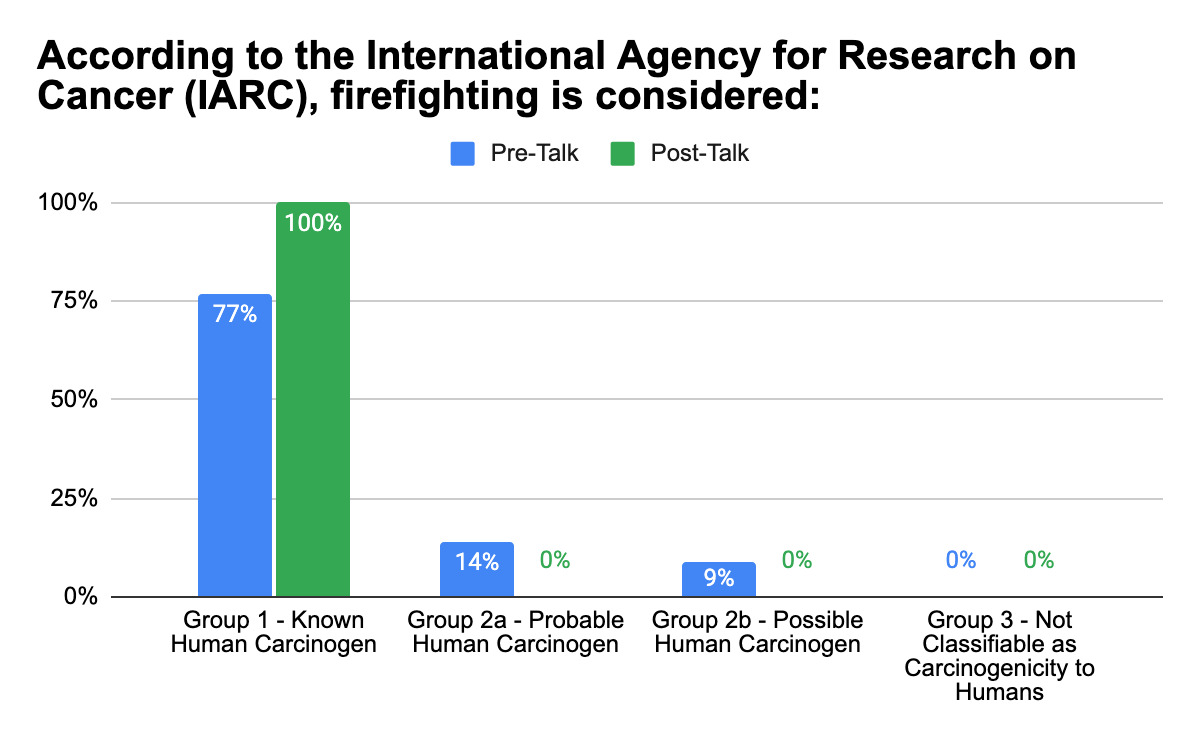
Mean knowledge scores increased from fifty percent prior to the educational intervention to seventy percent following the intervention (p = 0.00004; ninety-five percent confidence interval). The proportion of participants who correctly identified cancer as the leading cause of line-of-duty death among firefighters increased from seventy-eight percent pre-intervention to one hundred percent post-intervention (p = 0.00095). Recognition of firefighting as a Group 1 human carcinogen according to the International Agency for Research on Cancer increased from seventy-four percent to one hundred percent (p = 0.0019).10
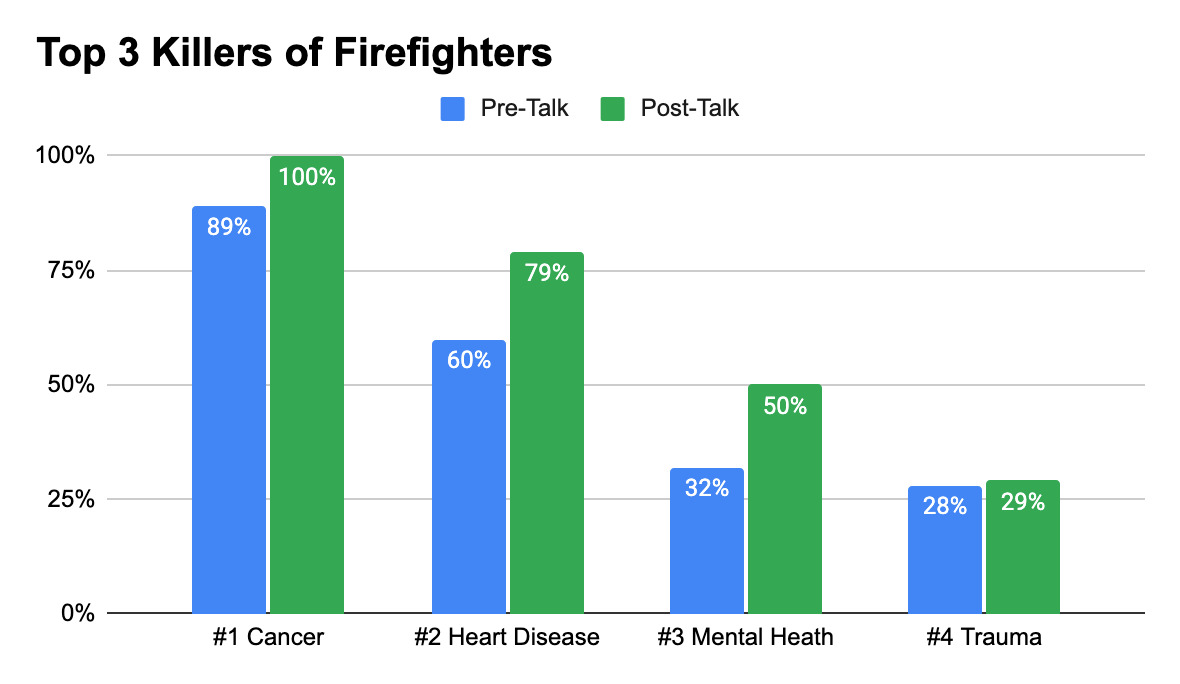
Prior to the intervention, eighty-nine percent of participants identified cancer as one of the top causes of firefighter mortality, compared with one hundred percent following the intervention (p = 0.36).
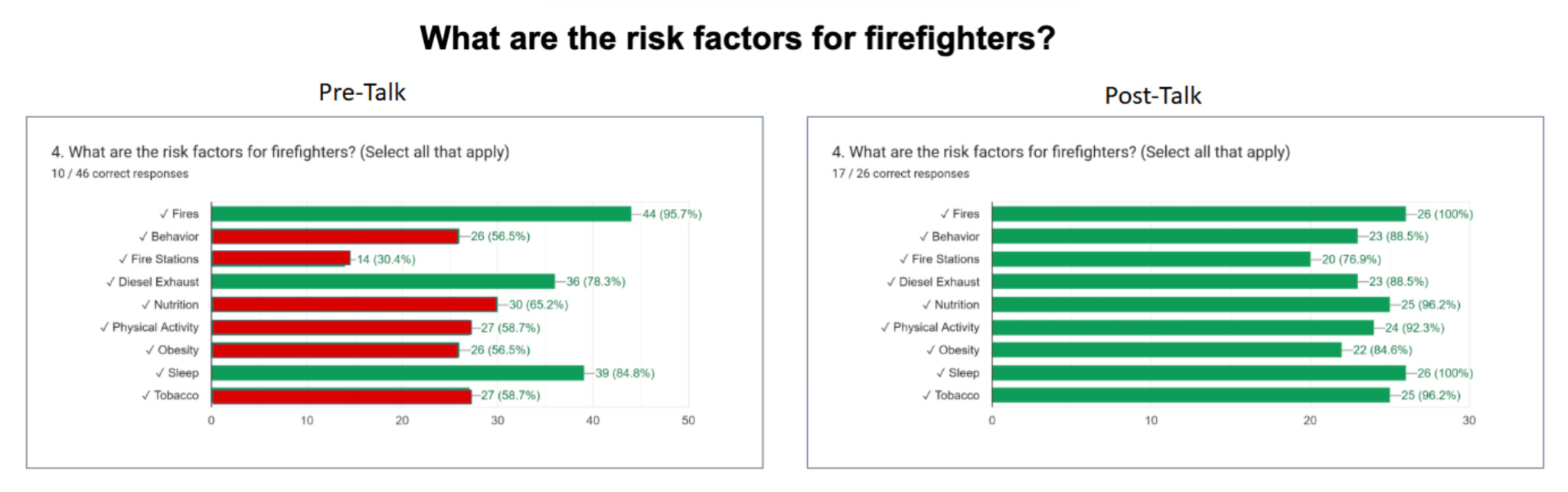
With respect to occupational cancer risk factors, participants correctly identified a mean of two of nine risk factors prior to the intervention and nine of nine risk factors following the intervention. Significant improvements were observed for identification of fire station exposure (p = 0.00007), nutrition-related risk (p = 0.0003), physical activity (p = 0.0004), obesity (p = 0.008), sleep disruption (p = 0.007), and tobacco use (p = 0.00003). No statistically significant change was observed for fire exposure (p = 0.16) or diesel exhaust exposure (p = 0.25).
Attitudes and Behaviors
On a five-point Likert scale, participants reported frequent screening for occupation (mean score, four of five) and rated occupational screening as important (mean score, 4.57 of five). Following the intervention, participants reported a mean comfort level of four of five when caring for patients overall and 3.85 of five when caring specifically for firefighter patients.
Post-Intervention Feedback
All participants agreed or strongly agreed that the educational lecture was helpful. Ninety-one percent agreed or strongly agreed that they intended to implement the information into their clinical practice when caring for firefighters.
DISCUSSION
Cancer in the fire service is apparent; however, many of the risk factors are modifiable and can be mitigated through targeted education and prevention efforts. The educational lecture provided highlighted the epidemiology of firefighter cancer, including discussion about firefighters having a greater risk of multiple types and more aggressive types of cancer. Modifiable and non-modifiable risk factors were also explained in relation to behavior, obesity, physical activity, sleep, and tobacco use. Potential solutions for reducing the risk of cancer were shared, including applying sunscreen, maintaining a healthy lifestyle, and offering methods for exposure tracking for firefighters. Finally, firefighter-specific cancer prevention recommendations, extending beyond USPSTF guidelines, were given to PCPs for both male and female firefighters.
This quality improvement study demonstrated that a brief, targeted educational intervention was associated with significant improvements in health care provider knowledge related to firefighter occupational cancer risk. In particular, gains were observed in recognition of firefighting as a carcinogenic occupation and in identification of modifiable occupational and lifestyle-related cancer risk factors.
The improvement in knowledge regarding sleep disruption, nutrition, physical activity, obesity, and tobacco use is clinically relevant for family medicine practice. These factors represent actionable targets for preventive counseling that extend beyond acute occupational exposures and align with the holistic, longitudinal approach central to primary care. Enhanced awareness of these risk factors and occupational differences in firefighter cancer screening may support more comprehensive cancer prevention discussions and support earlier identification of malignancies in this population.
Participants in this study practiced in a retiree firefighter clinic, suggesting that baseline familiarity with firefighter health issues may have been higher than in the general primary care population. Despite this, substantial knowledge gaps were identified prior to the intervention, underscoring the need for firefighter-specific education even in specialized practice settings. The magnitude of improvement observed suggests that similar or greater gains may be achievable in broader primary care environments.
Additional findings further support the potential impact of targeted education. Participants reported high perceived importance of occupational screening and increased confidence in caring for firefighter patients. The high proportion of clinicians expressing intent to incorporate the information into practice suggests that brief educational interventions may influence not only knowledge but also clinical behavior.
The consistently positive feedback highlights a broader unmet need for structured educational resources addressing firefighter occupational cancer risk. Requests for additional time and supporting materials suggest that while brief interventions are effective, they may be most impactful when paired with longitudinal educational strategies or reference tools integrated into routine clinical practice.
Limitations
This study was limited by its single-center design and modest post-intervention response rate. Outcomes relied on self-reported measures and did not assess long-term knowledge retention or objective changes in clinical practice. Future studies should evaluate sustained behavior change and patient-level outcomes associated with provider education. Additionally, participant attrition between pre- and post-intervention surveys and the inability to link responses to limited paired analysis may reflect a more motivated subset of participants, introducing potential for selection bias and overestimation of knowledge gains. Future studies should also incorporate unique identifiers to promote longitudinal assessment and strategies to minimize survey dropout in order to strengthen the study.
CONCLUSION
A brief educational lecture significantly improved health care provider knowledge and attitudes regarding firefighter occupational cancer risk. Incorporating firefighter-specific occupational health education into family medicine settings may enhance cancer prevention and screening efforts and represent a scalable strategy to improve care for this high-risk population.
This educational approach is likely to become increasingly important as policy initiatives expand firefighter cancer screening efforts. In Texas, House Bill 198, signed into law in May 2025 as the Wade Cannon Act, mandates that cities and municipalities provide cancer screening at no cost to firefighters beginning the fifth year of the firefighter’s employment and annually thereafter.17