

BACKGROUND
Colovaginal fistula often presents subtly but can be diagnosed through careful history and physical examination making it a key condition for clinicians to recognize in older adults with a previous hysterectomy. Because primary care physicians are often the first point of contact for patients noticing potentially embarrassing symptoms, they can make an early diagnosis leading to improved quality of life. A fistula is a connection between two epithelialized surfaces that is abnormal. In the case of colovaginal fistula, an abnormal communication between the colon and vagina exists allowing fecal matter and flatus to pass from the high-pressure bacteria-rich environment of the colon into the low-pressure environment of the vaginal canal. While colovaginal fistulas remain extremely rare, they are the third most common lower reproductive tract fistulas in women.1 During 1979 to 2006, the rate of colovaginal fistula was measured by looking at the rate of colovaginal fistula repairs.2 The rate was found to be 0.6 repairs per 100,000 women per year.2 The symptoms of colovaginal fistula are severe and warrant early detection and intervention. In addition to debilitation of the patient, colovaginal fistulas can cause severe complications such sepsis and malnutrition. In this case, the patient underwent surgery within two weeks of initial diagnosis.
CASE REPORT
A 79-year-old woman with a past medical history of Cesarean-section and hysterectomy presented to her primary care physician with a sensation of fluid in the abdomen, foul-smelling discharge, and vaginal flatus persisting for several weeks.
On physical examination, the patient’s vital signs were within normal limits and the abdominal exam showed a lower midline incision scar from previous Cesarean-section. On palpation, the abdomen was found to be soft and doughy. On pelvic exam, foul-smelling purulent discharge was noted, but there was not direct visualization of the colovaginal fistula itself. Based on this clinical picture, colovaginal fistula was considered as part of the differential diagnosis and the patient was referred for imaging and to a general surgeon.
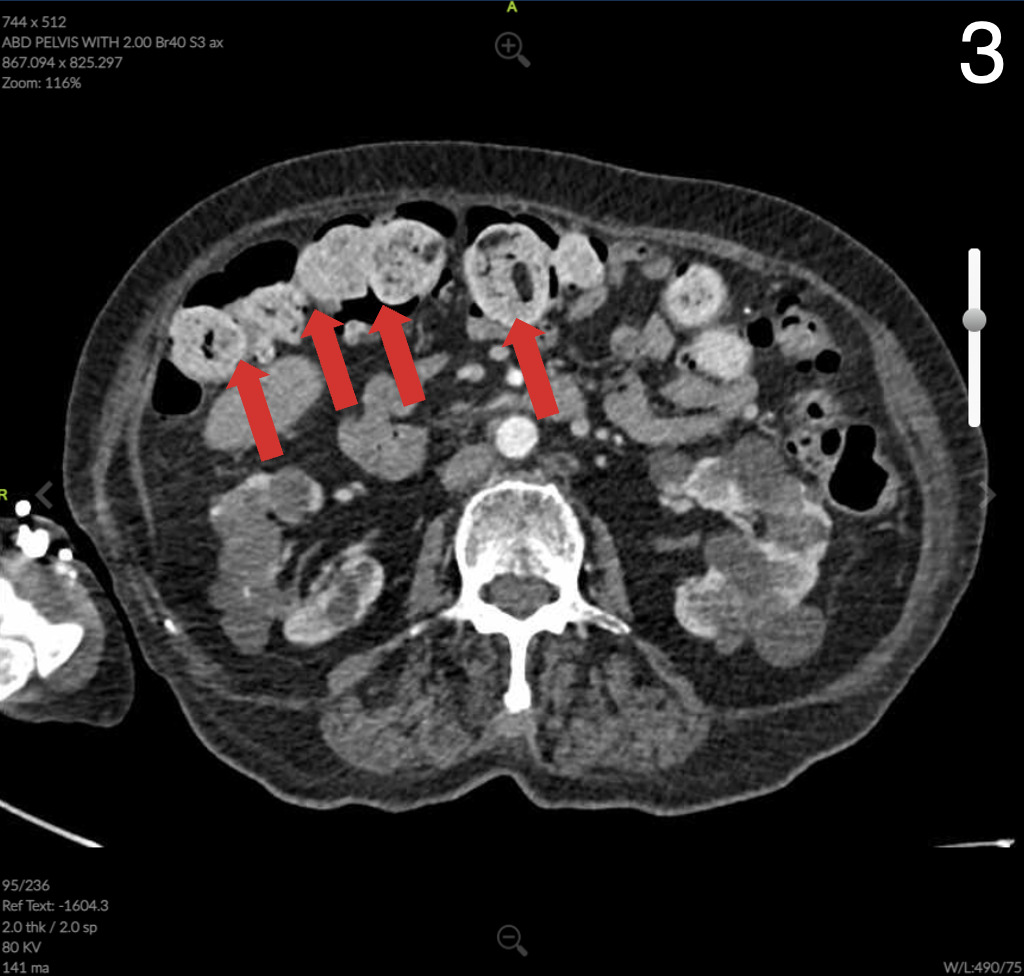
Computed Tomography (CT) of the abdomen and pelvis showed colonic wall thickening particularly in the pelvis close to the vaginal vault. A colonoscopy revealed a severe kink that could not be crossed in the sigmoid colon and extensive diverticular disease.



The patient was referred to a general surgeon for low anterior resection of colovaginal fistulous connection and primary colon anastomosis between segments of healthy colon. The patient was noted to have widespread pelvic adhesions and scarring. The opening in the vagina due to the fistula was left to close naturally. The patient was discharged on post-op day three with no complications. Three months postoperatively, the patient reported no vaginal discharge. The incisions healed well with no signs of infection.
DISCUSSION
Pathology of the colonic portion of colovaginal fistula revealed severe acute on chronic diverticulitis with stricture, perforation, and fibrinous serositis with adhesions consistent with clinical history of colovaginal fistula negative for dysplasia or malignancy. The anastomotic donuts were benign and viable colonic mucosa was negative for dysplasia or malignancy. Review of microbiology of the vaginal canal revealed detection of only normal vaginal flora that was negative for G. vaginalis, T. vaginalis, N. gonorrhoeae, C. trachomatis, and C. albincans.
CONCLUSION
Past medical history and comorbid conditions that are often associated with colovaginal fistula such as diverticular disease, previous hysterectomy, inflammatory bowel disease, pelvic trauma, or pelvic radiation should heighten clinical suspicion of colovaginal fistula when combined with symptoms of vaginal flatus, malodorous discharge, or fecaluria.4 Often the first symptom noted by the patient will be passage of flatus through the vagina. While symptoms may be intermittent, the full clinical picture of vaginal flatus, persistent foul-smelling vaginal discharge, passage of stool through the vagina, with or without pelvic pain should give rise to a diagnosis of colovaginal fistula as the patient may have been waiting to seek care due to embarrassing nature of symptoms being experienced. It is also important to note how patient language may point to symptoms such as in this case where the patient reported a “rush of fluid from the vagina” upon bending to pick up an item. Noticing subtle language can be helpful to clinicians in their history taking and final diagnosis. As for the physical exam, feculent discharge in the vaginal vault and repeated failure of treatment of vaginitis should raise concern for colovaginal fistula development. Clinicians should be aware of the gradual progression of colovaginal fistula formation, the role of diverticular disease as a common etiology, and the anatomical proximity of the colon to the vagina after a hysterectomy that leads to increased risk. Colovaginal fistula can present with non-specific symptoms that can be diagnosed through history and physical examination leading to early intervention. Primary care physicians play a critical role in early diagnosis leading to successful repair and quality of life even for a patient with advanced development of adhesions.
ACKNOWLEDGMENTS
Thank you to the staff at Huntsville Memorial Hospital and Texas Surgery Center Huntsville including the radiology and pathology departments.