INTRODUCTION
GLP-1 RA such as semaglutide and tirzepatide have found increasing use for weight management due to potent effects on weight reduction through delayed gastric emptying and appetite modulation. Several reviews reveal consistent efficacy in reducing body weight compared with placebo across multiple randomized controlled trials.1
Despite growing adoption and inclusion in global guidelines recognizing obesity as a chronic disease requiring extended management, evidence on outcomes after cessation of GLP-1 therapy is limited and heterogeneous. Importantly, current literature does not thoroughly explore the relationship between treatment duration and propensity for weight regain.2,3
This project will extend the literature through an exploration of weight trajectories after cessation of long-term GLP-1 RA therapy and specifically seeks to answer the question: is there a duration of treatment with GLP-1 RA therapy after which weight loss is durable? This addresses a facet of GLP-1 RA therapy that has not been delineated completely.
METHODS
Study design and data source
We conducted a retrospective observational analysis of real-world prescribing and weight data for patients treated with GLP-1 RA for weight management. Data were derived from de-identified electronic health record (EHR) extracts including medication orders, patient demographics, and longitudinal weight measurements.
Cohort construction and de-identification
Adults >18 years started on semaglutide or tirzepatide between 1/1/2005-7/26/2025 were analyzed.
All patient identifiers were removed prior to analysis, with medical record numbers replaced by unique study identifiers. Medication orders lacking structured information on total days supplied were excluded, as these were frequently free-text entries unsuitable for reliable longitudinal analysis. Drug names and strengths were parsed and standardized using a custom cleaning function to extract numeric dose information.
Orders for oral semaglutide (Rybelsus) were excluded due to low frequency and its limited indication for weight loss.
Definition of therapy courses
Medication orders were aggregated into discrete “courses of therapy.” For a given patient and drug, multiple orders were considered part of the same course if the gap between the end of one order and the start of the next was ≤30 days. Orders separated by more than 30 days were classified as distinct therapy courses.
Courses were required to include evidence of dose escalation (i.e., multiple strengths) to reduce inclusion of very short or incomplete treatment attempts. Courses with insufficient spacing (<365 days) between consecutive courses for the same patient were excluded to ensure adequate post-therapy follow-up.
Weight measurements
Weight measurements recorded during active therapy were linked to each course if they occurred within the therapy interval. Post-therapy weight measurements were identified within approximately one year following therapy cessation. Courses were retained if at least one post-therapy weight measurement was available within this window.
For analyses focused on one-year outcomes, post-therapy weight change was calculated relative to the weight recorded at the end of therapy. Percent weight change was calculated using end-of-therapy weight as the reference.
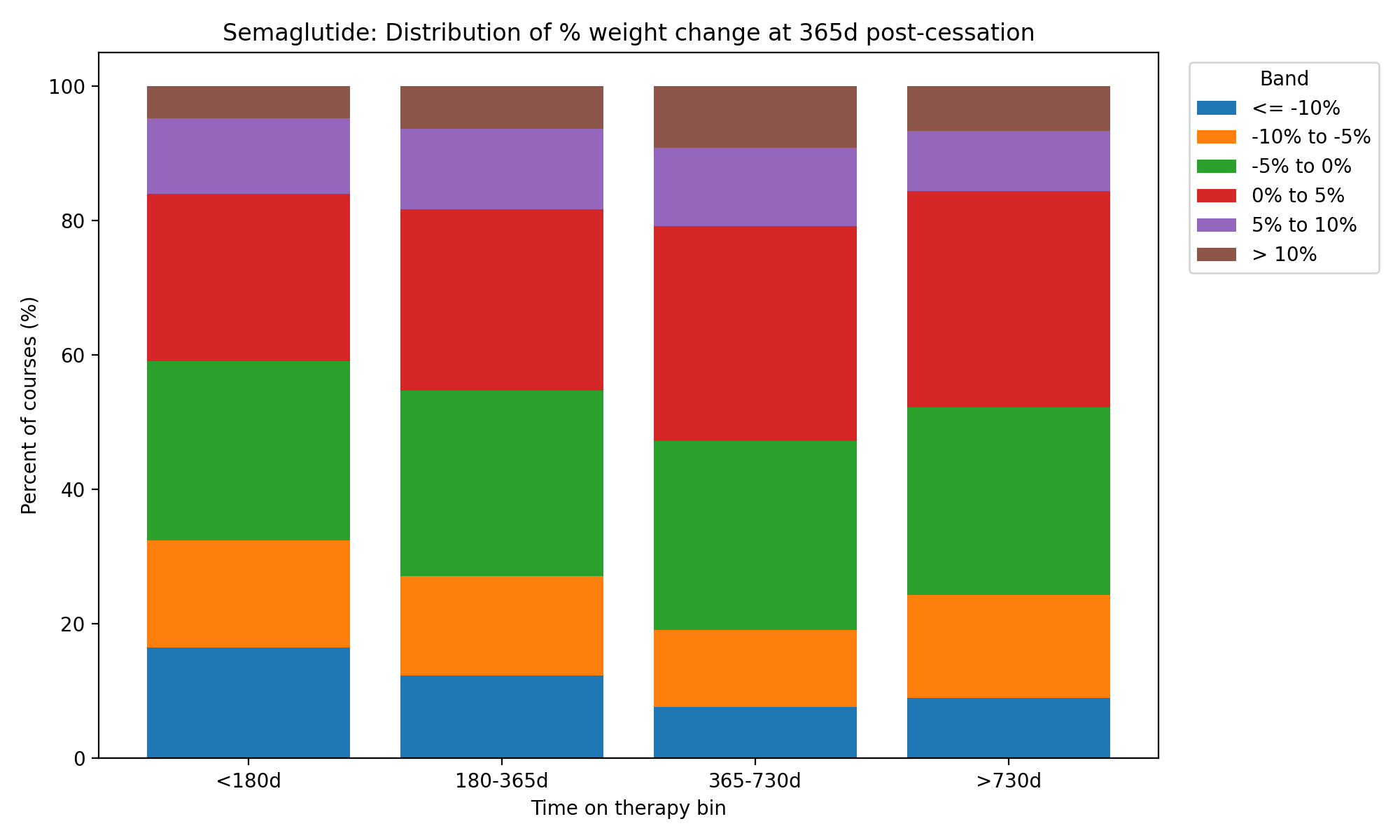
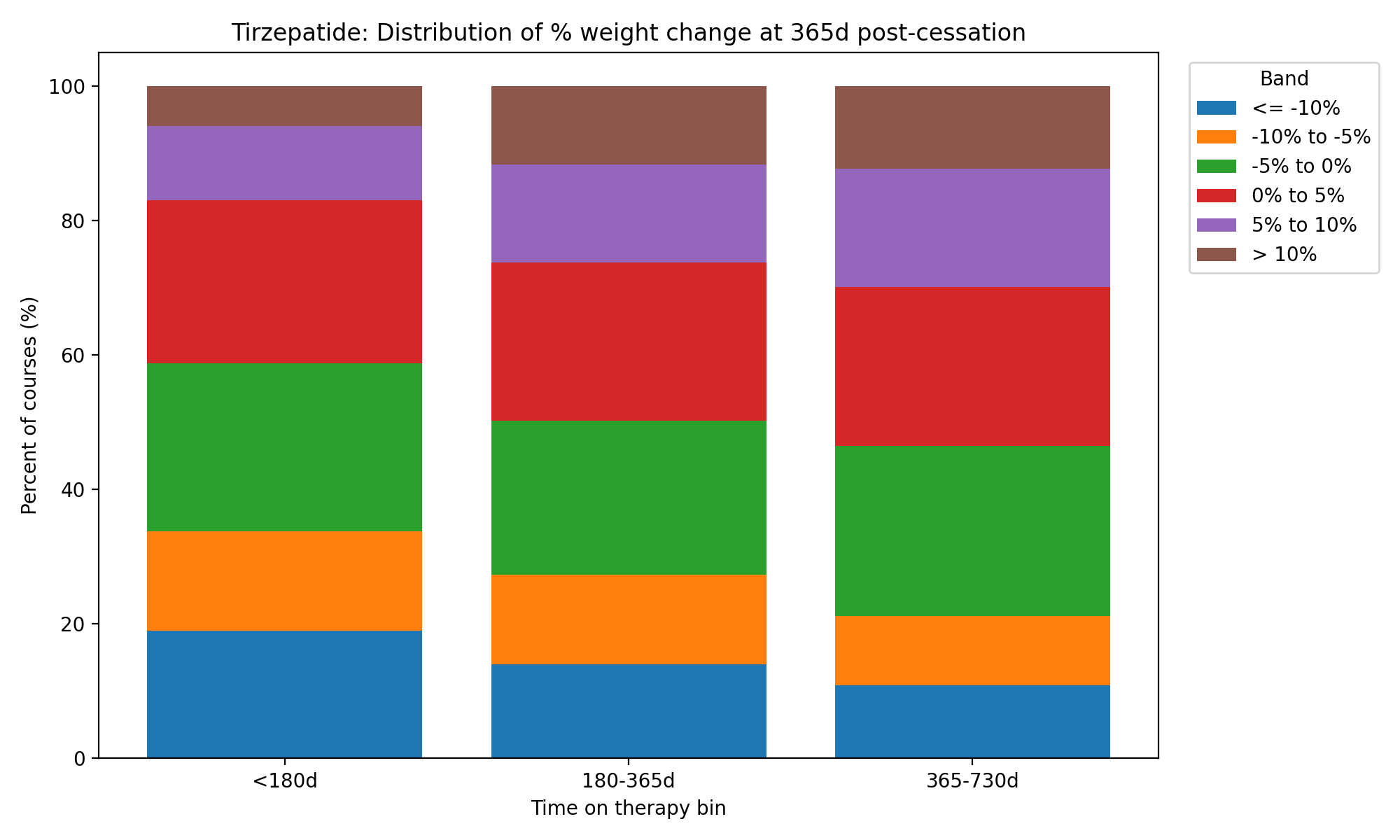
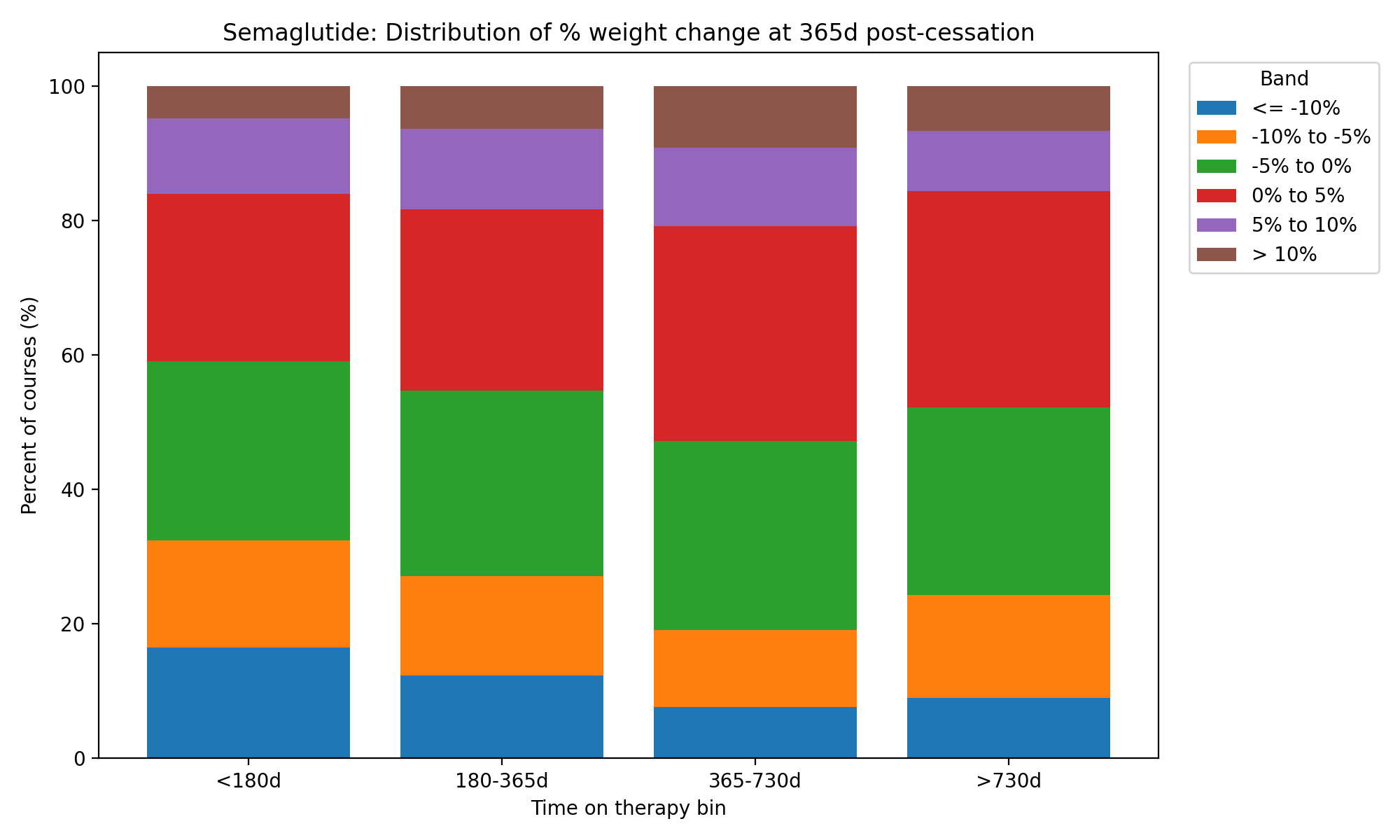
Therapy courses were stratified by duration of treatment into predefined bins (<180 days, 180–365 days, 365–730 days, and >730 days). Semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) were analyzed separately due to known differences in dosing and magnitude of weight loss.
Outcomes
Primary outcomes included absolute and percent weight change approximately one year after therapy cessation. Secondary descriptive measures included therapy duration, ending dose strength, number of weight measurements, and availability of post-therapy follow-up.
Statistical analysis
Descriptive statistics were used to summarize demographics, therapy characteristics, and weight outcomes across therapy duration groups.
Mixed-effects regression analyses incorporating therapy duration and time since cessation as predictors of weight change were also performed.
All analyses were performed using reproducible data-processing scripts, with drug-specific analyses conducted independently.
RESULTS
Table 2 and Table 3 show case the weight change based on therapy duration after cessation at the 1-year post cessation time point. Interestingly, we found in our data that the groups with short term therapy of <180d continued to lose weight through the first year of cessation with semaglutide group losing an additional 2.35% body weight and tirzepatide group losing an additional 2.85% of body weight. This was felt to be an erroneous finding related to the study’s design; this is a purely retrospective study looking at medication orders and weights. There is no verification of start and stop dates of the medication. Therefore, subsequent aspects of the analyses looked at subsets of the data with longer therapy durations which may have reflected a more genuine post therapy cessation weight delta.
As seen in Figure 1 and 2, there is a distribution of weight change after cessation of GLP1-RA therapy; some patients maintain their weight loss, some regain weight, and some continue to lose weight. Excepting the <180d therapy duration given its anomalous findings, there is a trend towards an increased proportion of patients regaining weight with longer therapy duration, particularly in the tirzepatide group.

Mixed effects analysis is the primary statistical test used to answer the principal question of the study. Using the available post treatment weights at varying time points per patient, the mixed effects analysis enabled us to look at the data more broadly as opposed to the categorization approach undertaken thus far. This analysis revealed that there was not a significant or consistent relationship between treatment duration and post cessation weight regain. If anything, a trend towards increased weight gain was noted with a longer duration of therapy.
Multiple mixed effects analyses were undertaken after the one focusing on all the data available. Subsets of the data based on drug and time on treatment were analyzed independently given the anomalous data with short durations of therapy. Even then, the mixed effects analyses did not reveal a significant durability of weight loss with longer durations of therapy.
DISCUSSION
Our project had some significant limitations due to the study design. Principally, there was no way to verify whether medication orders lined up with patients actually taking the medication. This concern would always be there with questions of patient noncompliance, but this study design in particular lends itself to this type of error. As such, some results were felt to be inaccurate with patients on GLP-1 RA therapy for very short durations being seen to continue to lose weight after cessation. We felt this more likely reflected a switch to alternate sources of the therapy such as through compounding pharmacies or cheaper online based weight loss prescribers. This was despite the methodological choice to only include patients with multiple orders for the medication to try and select for patients who were more likely to be taking the drug; this choice may have helped avoid patients unable to access the drug due to insurance issues after initial order, but did nothing to address the question of people getting access through alternate sources external to our system.
With this aside in mind, we can focus our discussion on the patients treated for a longer duration of time. We have found that for these patients there is a trend towards increased weight gain after therapy cessation despite the longer duration of therapy. This can be seen in the descriptive analyses and table 2 and 3 as well as figures 1 and 2 and the coefficients of the mixed effects models summarized in table 4. Particularly for tirzepatide, in the mixed effects model on a subset of the data with therapy duration greater than 180 days, there is a positive coefficient with therapy duration and weight regain after cessation with a significant P value. The overall mixed effects model included all available therapy courses, numbering over 6000, and had a positive coefficient for the relationship between therapy duration and weight regain after cessation and reached statistical significance. Although the study is limited in the ways defined above, this cohort is larger than many of the key meta-analyses seen in the literature today. With the implicit validity of these data given the expected weight regain seen after therapy cessation, there is some credence to the idea that this is a genuine reflection of nondurability of weight loss with GLP-1 receptor agonist therapy.
The question of the effectiveness of GLP–1 RAs and the knock-on effects of weight loss in better health outcomes has been well answered.1 This study sought to glean insight towards defining an endpoint of GLP–1 RA therapy. Despite the limitations, these data suggest that long term therapy is not associated with durable weight loss with withdrawal of the medication and supports guidelines for extended therapy.2 However, it remains evident that different people respond differently to withdrawal with a subset of the population maintaining weight loss even after cessation of therapy.