Section 1. Introduction
Manor Free Clinic (MFC) is a community-based clinic that provides no-cost primary and urgent care to uninsured patients. Implemented in an elementary school in Manor, a suburb of Austin, Texas, the clinic serves patients from more than 23 neighboring zip codes. In 2025, the clinic served over 200 uninsured patients, most of whom are low-income, immigrants, and/or from minority communities. Community clinics can often lack structured mechanisms to capture patient feedback,1 and there is limited evidence on how patients experience mutual-aid models, particularly those integrating social determinants of health (SDoH) into real-time care. To address this gap, this study used a mixed-methods approach to evaluate patient experiences at MFC to identify quality improvement opportunities and uplift patients’ voices.
Sustainably addressing the health of systemically disadvantaged communities requires going beyond medical care alone. Housing, food security, transportation, insurance barriers, education, legal barriers, and economic stability all profoundly shape how someone interacts with healthcare and their health outcomes.2 MFC addresses SDoH alongside medical care through two main ways: the clinic’s “Resource and Education Room” and its mutual-aid principles.
At MFC, one visit consists of three distinct stages: 1) Interview Room, where SDoH screening is conducted, 2) Provider Room, where medical care is provided, and 3) Resource and Education Room, where patients receive education on medical diagnoses and prescriptions, along with tailored resource linkage. Based on the SDoH screening results, the services range from over-the-counter medications and service vouchers to insurance eligibility screening. All patients conclude their visit here, standardizing the social encounter and underscoring the value of addressing social needs. The designated physical space also enables private, unhurried conversation. These slower-paced conversations allow patients and clinicians to be more responsive and accountable in the care plan, ultimately leading to an improved quality of care.3
The values of mutual aid underscore the entirety of MFC’s model. Historically, community run clinics tended to have a unidirectional charity framework that is often disempowering to those receiving care. Instead, mutual aid clinics focus on cultivating reciprocal care between volunteers and patients in order to foster solidarity.4 MFC was founded by members of the Manor community for its most underserved, and all the volunteers come from surrounding areas. Patients are partners in the clinic’s model; they are invited to volunteer and be involved in the clinic’s workings. At the same time, providing patients with the autonomy to have their voice heard separate from the often stressful clinical environment leads to a more complete and unhurried setting to truly hear patients’ stories.5 The first step in cultivating this space for patient voices begins with surveying patients willing to share their feedback and story with the clinic.
Section 2. Methods
Survey participants included patients who had visited MFC between November 2025 and March 2026 (n = 29). All patients completed the three parts of the clinic visit and were offered the option of completing an anonymous paper survey at the end of their encounter in the “Resource and Education Room.” Volunteers were instructed to verbally screen for past survey participation to prevent duplicate submissions. Respondents could also opt into open-ended written feedback or a follow-up interview at the end of the survey. Semi-structured qualitative interviews were scheduled and conducted at a later date over phone or in-person, and transcripts were made from the interview recordings (n = 5). The surveys and interviews were available in either English or Spanish. Responses in Spanish were translated to English for analysis. Participation in either were voluntary, and the responses were collected anonymously. Interview participants were compensated with a gift card to a local grocery chain.
The objectives were to 1) create a culture of gathering patient feedback by incorporating it into clinic workflow, 2) collect satisfaction-related metrics and in-depth qualitative feedback, and 3) identify areas of improvement.
Section 3. Results
The paper survey included a multiple choice question about which of the 10 services were utilized and five-point Likert scale questions about satisfaction with each visit step (see Figure 1). The open-ended section followed immediately after the ratings and focused on favorable aspects and/or improvement suggestions. Using a mixed methods approach, open-ended interview questions were developed to be consistent with the content and order of the paper survey. The interview questions gave respondents the opportunity to provide in-depth feedback on survey responses, directly connecting the quantitative scores to qualitative themes and developing a holistic picture of the patient experience. Other topics relevant to clinic evaluation such as healthcare access other than MFC and the role of MFC in the community were also asked about during the interview. Survey data was analyzed using descriptive statistics, and interviews were analyzed using affinity mapping and thematic analysis.
Survey Results
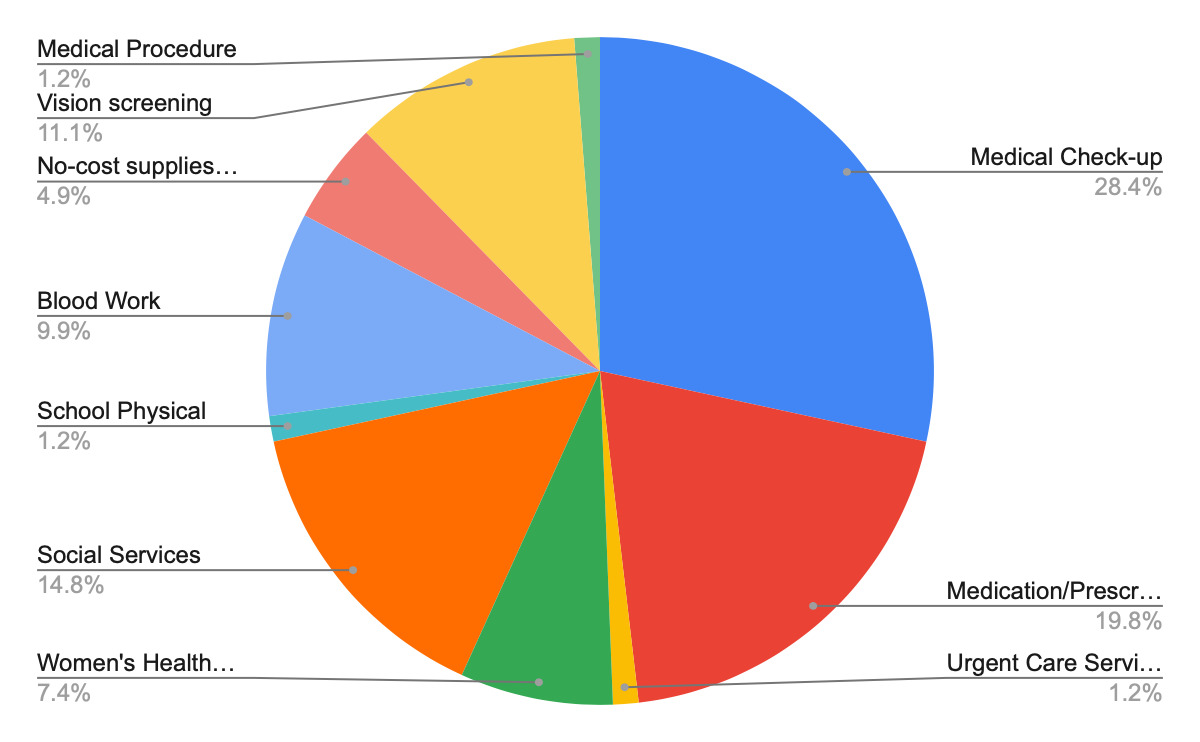
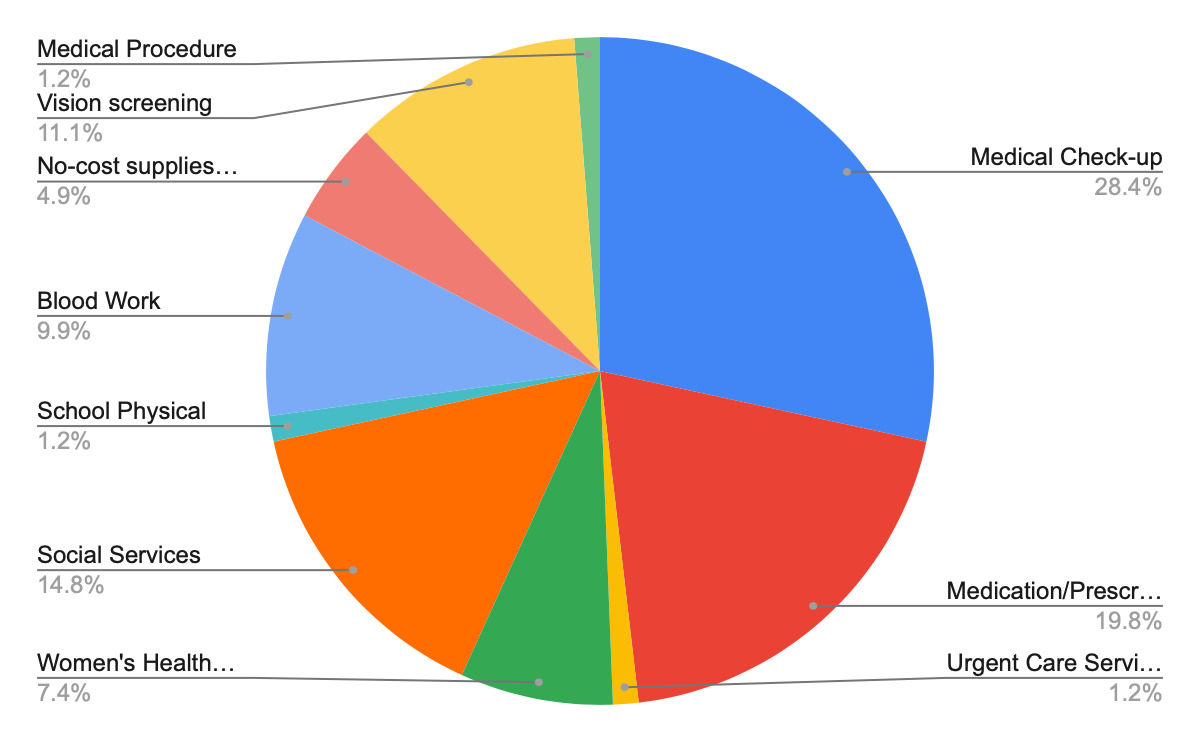
Among the 29 responses, 81 total services were utilized and an average of 2.79 services per patient were utilized. 72% of respondents received multiple services. The most common services included check-ups (79%), medication prescriptions (55%), and social services (38%) (See Figure 2).
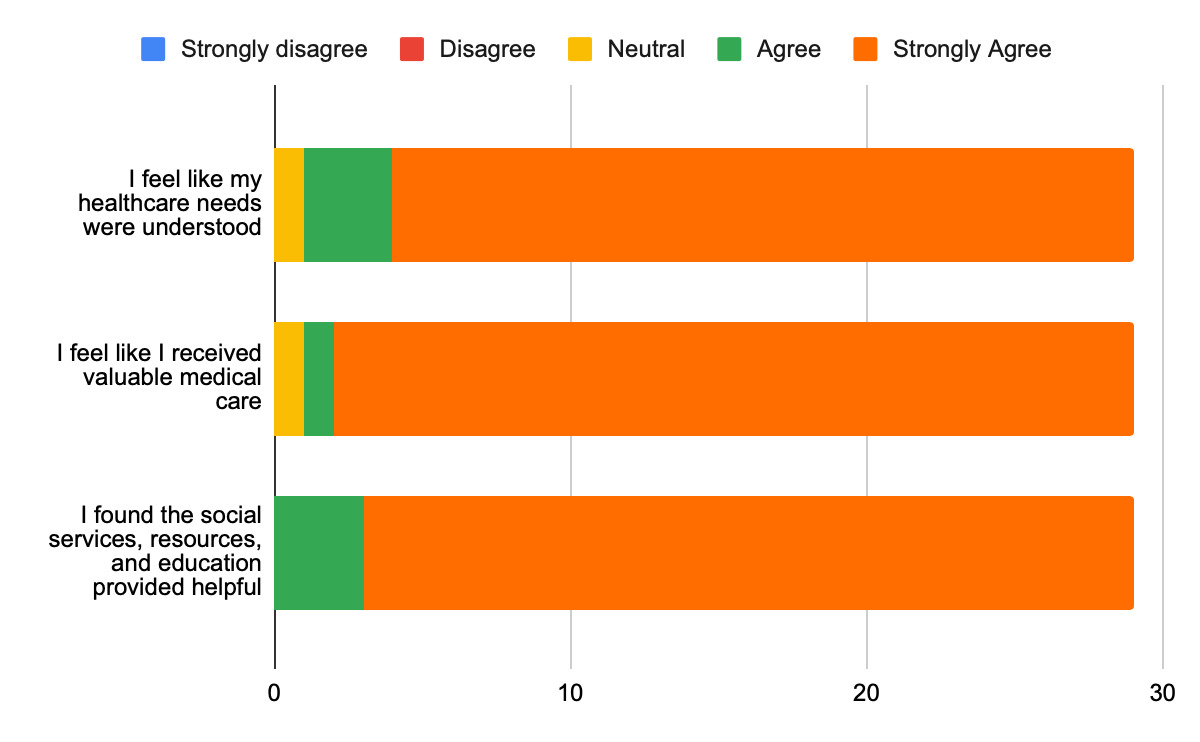
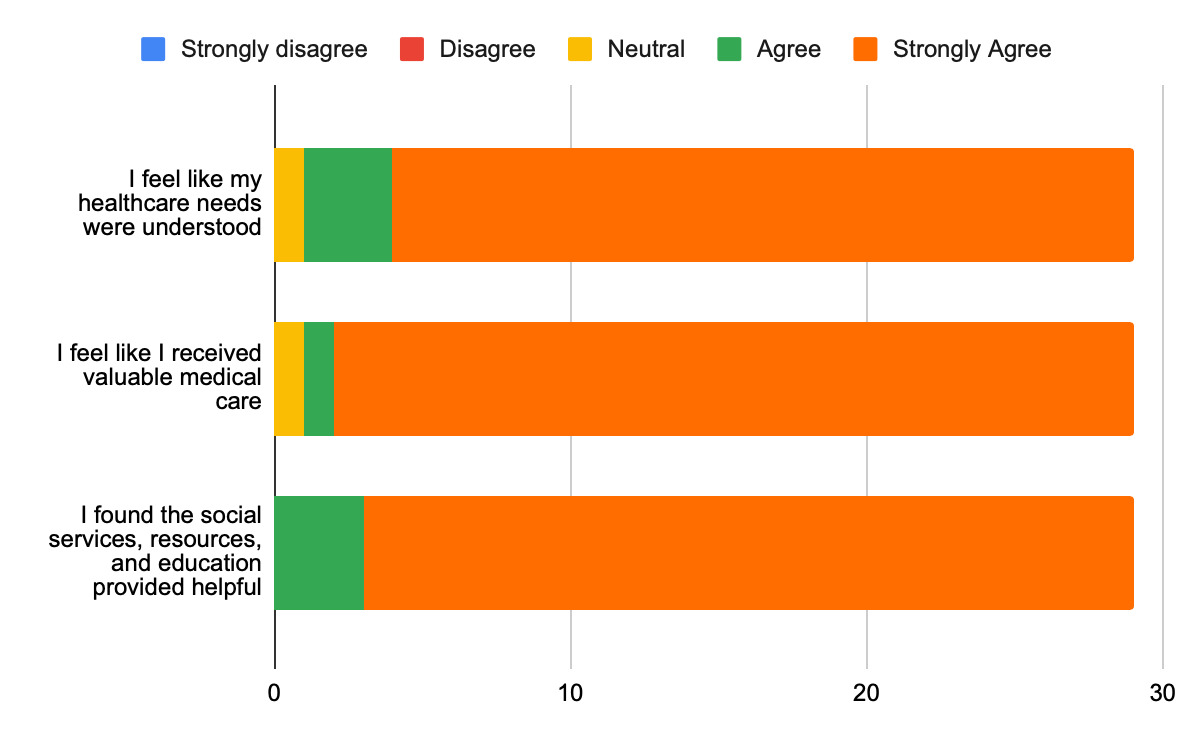
Overall satisfaction was high with 82% of respondents rating their visit as ‘Excellent’ and 18% rating it as ‘Very Good.’ Satisfaction with each of the visit steps were also overwhelmingly positive (See Figure 3).
93% of respondents understood the information that was provided to them. 93% of respondents would visit Manor Free Clinic again and 97% would recommend the clinic to others. The open-ended responses were brief yet direct, highlighting respectful treatment, supportive staff, and clear communication along with recommendations to improve vital signs equipment and patient-centered communication.
Interview Results
All five interview participants identified as residents of Manor, or surrounding areas, with approximately half identifying as having international origins. Most participants had limited prior engagement with Manor Free Clinic, with four reporting one or two visits. Participants learned about MFC through a mix of informal and formal channels; three participants cited word-of-mouth referrals from community members, while two reported learning about the clinic through marketing sources, such as flyers or Google Maps. Transportation to the clinic was largely self-managed, with most participants driving themselves; one participant relied on a family member for transportation.
All participants reported relying exclusively on MFC for their current healthcare needs due to affordability constraints and lack of insurance coverage. Several participants referenced prior access to healthcare through insurance (more than two years prior), highlighting a transition from insured to uninsured status. Across interviews, participants consistently identified systemic barriers to healthcare access, such as high costs and financial constraints. One patient explained, “It’s too expensive… I only go if I really feel like I needed to…if not, I normally just power through whatever is happening.” Another participant stated that “…my job doesn’t offer healthcare…it costs too much to get it privately.” In addition to these systemic barriers, the desire for a consistent provider who builds trust and provides continuous care emerged as a recurring theme. One participant shared, “I never had a consistent doctor; it has always been different doctors. I guess that helps because maybe they know your history.”
Clinic Strengths
Participants expressed strongly positive sentiments toward MFC. Many described the clinic as exceeding expectations, particularly given its free services. When asked what aspects of clinic patients liked, one participant originally stated in Spanish, “Everything - the first time, I was so surprised. They did so many tests and they were all so nice…. It was so surprising that I didn’t have to pay. The fact that they don’t discriminate and it is all free was just amazing.”
Key strengths identified included:
-
Interpersonal care: Participants consistently emphasized feeling “seen”, heard, and respected by providers and volunteers. The perceived willingness of staff to spend time and communicate thoroughly was a defining feature of the experience.
-
Continuity and coordination: Patients appreciated the smooth flow between clinic stages, noting that they were not required to repeatedly share the same information.
-
Environment: Cleanliness and organization were frequently highlighted.
-
Accessibility and affordability: Participants expressed gratitude for free or reduced-cost healthcare services located conveniently in the community, including prescriptions obtained through Manor Pharmacy.
-
Hospitality: Small touches, such as free coffee, contributed positively to the overall experience.
-
Free and relevant health supplies: Patients enjoyed getting free supplies related to their care (e.g. blood cuff monitor given to patients with high blood pressure)
-
Breadth of services: Some participants were pleasantly surprised by the range of tests and services offered.
Participants also described MFC as a critical community resource that addresses unmet healthcare needs and provides accessible care. Many expressed deep gratitude and appreciation for the clinic and its volunteers. Patients reported leaving visits feeling more informed about their health and empowered to take next steps, with one patient sharing “I am so grateful. In part, my health was so bad with my leg and the clinic let me in and taught me how to get better. I just wasn’t expecting this. Thank god I was able to leave with a better leg and with medications.”
Clinic Pain Points and Improvement Opportunities
During the qualitative interviews, participants were asked to reflect on aspects of the MFC clinic experience they disliked, found uncomfortable, or would change. Participant responses identified pain points, followed by opportunities for improvement.
Key pain points identified include:
-
Inconsistent use of preferred pronouns during patient interactions: Misuse of preferred pronouns, led to one patient being unclear on the rationale for collecting this information.
-
Wayfinding and signage: Difficulty locating the clinic entrance from the road or parking area without assistance.
-
Wait times: Lack of clarity around expected wait times overall and between clinic stages.
-
Administrative processes: Technical issues (e.g., printer malfunction) causing delays.
-
Privacy concerns: While generally acceptable, some participants noted limited privacy during conversations in provider and resource rooms.
-
Irrelevant health supplies: Patient felt awkward being offered free health supplies that weren’t relevant to their needs or care.
-
Insurance screening interactions: Mixed experiences with the MAP (Medical Access Program) qualification process, with some participants finding it awkward when they anticipated ineligibility, while others found it helpful.
These findings point to several opportunities to enhance the MFC experience. Participants emphasized the need to expand clinic capacity through increased frequency, physical space, and staffing to better meet demand, improve wait-time comfort, and allow for more private conversations. One participant explained that a larger space would facilitate more private patient interactions, “I’m just saying so y’all can be able to work and, you know, nobody listens to nobody’s conversation”. Improved communication channels, such as access to a phone number or website for post-visit follow-up, were also recommended. Additionally, participants called for clearer wayfinding through more visible signage and more tailored distribution of free supplies to better align with individual patient needs.
Importantly, even as participants identified these areas for improvement, they expressed strong appreciation for the care they received. As one participant shared, "People are friendly and explain step by step, which is different compared to my country. People volunteer and do this for no money, so that’s great. I see their heart."
Section 4. Discussion
This study demonstrates that a mutual-aid clinic model with integrated SDoH intervention can achieve high patient satisfaction while delivering holistic, patient-centered care. Findings indicate that MFC delivers a highly valued and trusted experience for uninsured patients, becoming the primary healthcare for many. While operational and communication improvements are needed, the clinic’s patient-centered approach and volunteer-driven model are central to its success and perceived value within the community. This approach contrasts with more common models of care, in which social needs are addressed through delayed referrals or not addressed at all.6 While dividing care into multiple visit steps can risk fragmentation, effective coordination across these stages appears to mitigate this concern, as patients highlight smooth transitions between steps. This finding aligns with existing evidence that continuity and communication are essential to patient-centered care, particularly in resource-limited settings.7
The Resource and Education Room represents a central innovation of this model. By combining patient education with same-visit resource navigation in a single, dedicated space, the clinic is able to maintain quality while maximizing efficiency. This allows patients to leave with both medical guidance and tangible support, as 93% of survey respondents reported a strong understanding of their care. This is consistent with prior literature demonstrating that social needs assistance is associated with improved patient satisfaction.8
Importantly, patient feedback in this study was not only descriptive but actionable. Qualitative interviews identified specific areas for improvement, including expanded capacity for patients, consistent pronoun use during patient interactions, wayfinding, wait time communication, improved post-visit communication channels, tailored free resource distribution, and enhancing conversational privacy. These findings demonstrate how patient feedback can serve as a practical tool for ongoing quality improvement rather than solely an evaluation measure.
This active integration of patient opinion strengthens the clinic’s mutual aid philosophy, which positions patients as active participants rather than passive recipients of care. Prior work has similarly shown that community participation in healthcare models is associated with increased patient empowerment and improved health outcomes.9 To communicate these results back to patients, we plan to develop and share clear, accessible summaries of initial patient feedback and key findings across multiple channels (e.g. in-clinic materials, digital updates on social media/website, and community forums). A plan will be drafted to continue a culture of soliciting patient feedback to engage patients in co-designing MFC improvements, while remaining transparent about what is changing, how current and future experiences will differ, and what patients can expect during the transition.
A tension emerged between the survey results and the qualitative interviews–while survey responses were extremely positive, interviews revealed more nuanced challenges. This underscores the limitations of relying solely on quantitative satisfaction metrics, which may obscure important aspects of patient experience. Prior research has questioned the ability of satisfaction surveys to fully capture quality of care,10 while more recent work emphasizes the value of qualitative methods in elevating patient perspectives and informing care delivery.11
These findings have relevance beyond MFC, particularly for free, community-based, and/or volunteer-run clinics operating with limited resources. Key components are readily transferable, including structured SDoH integration within clinic workflows and embedded patient feedback mechanisms. For example, clinics could incorporate a brief post-visit survey or designate a specific step in the visit for resource navigation. Together, these elements support a scalable approach to more holistic, patient-centered care and contribute to broader efforts in safety-net innovation.
Section 5. Limitations
This study’s small sample size (n = 29 surveys, n = 5 interviews) limits generalizability to other settings with different patient populations and resources. Selection bias was likely, as only patients who attended the clinic and chose to participate were included. Participants may have been more likely to respond if they had positive experiences, potentially overrepresenting satisfaction. 14 patients indicated interest in participating in interviews, but nine rescinded their interest due to timing constraints, or personal reasons. Social desirability bias may have also influenced responses given the volunteer-run, free care context. Additionally, the cross-sectional design captures experiences at a single time point and does not assess longitudinal outcomes. Language limitations may have restricted participation for some patients.
Section 6. Conclusion
Incorporating patient experience surveys and interviews within a mutual-aid clinic provides a practical approach to informing quality improvement. This study demonstrates that SDoH integration does not require large budgets or specialized infrastructure; it requires intentional design. By embedding resource navigation, patient education, and patient feedback directly into clinical workflows, mutual-aid clinics can deliver holistic care that patients trust, value, and return to. As safety-net clinics continue to face pressure to do more with less, MFC offers a concrete example of how community-driven care can deliver high quality and personable healthcare with low-cost solutions through creating a culture of soliciting patient feedback regularly. Combining qualitative and quantitative feedback captures a holistic view of the patient experience that normally isn’t captured in mutual aid clinics.1 Future work should expand sample size, incorporate longitudinal evaluation, and assess the impact of implemented changes to further refine and scale this approach, ultimately contributing to a growing evidence base for equity-centered, community-rooted healthcare.
Funding sources
None
Conflicts of Interest
None declared
IRB approval status
Not applicable