


BRIEF BACKGROUND
This case highlights the need for heightened clinical suspicion and advanced imaging when athletes present with focal scapular pain following direct impact during cricket fielding. Due to the rise in popularity of cricket in the United States, providers should familiarize themselves with common cricket injuries and their presentations in order to quickly and effectively treat patients. In this case, a 30-year-old male presented to the sports medicine clinic with left shoulder pain. He was playing in a recreational cricket match and fell down in an attempt to field a ball in play. He landed directly on his left shoulder and had since experienced significant pain and difficulty lifting his arm above his head. He described his pain as sharp with certain movements and occasionally shooting down to his upper arm. It did not reach into his forearm or hand. He had a history of a similar injury to his right shoulder that occurred in 2018 while playing cricket, which eventually improved with muscle strengthening exercises at the gym. However, this new injury prohibited the patient from exercising at the gym and inhibited certain movements.
CASE REPORT
Physical Exam
Left Upper Extremity Exam
Inspection of the extremity revealed no misalignment, scapular winging, or atrophy. The acromioclavicular prominence was normal with no swelling. There was no tenderness of the suprasternal notch, the clavicle, the coracoid process, the acromioclavicular joint, the bicipital groove, the scapula, or of the greater tuberosity upon bony palpation. Similarly, soft tissue palpation yielded no tenderness of the supraspinatus muscle, infraspinatus muscle, subacromial bursa, subdeltoid bursa, pectoralis major insertion, or glenohumeral joint region. Testing of active range of motion elicited painful external rotation at 90 degrees of shoulder abduction. Similarly, evaluation of passive range of motion resulted in painful external rotation at 90 degrees of shoulder abduction. Strength testing of the extremity showed adduction 5/5, flexion 5/5, extension 5/5, internal rotation 5/5, abduction 4/5, external rotation at 90 degrees of abduction 4/5. Special tests that were conducted that produced a negative result included the Hawkins test and Neer’s test, as well as the empty-can test. However, O’Brien’s test was positive and caused pain.
Differential Diagnosis
-
Left Rotator Cuff Tear / Tendonitis
-
Labral Tear of the Left Shoulder
-
Left Scapular Fracture
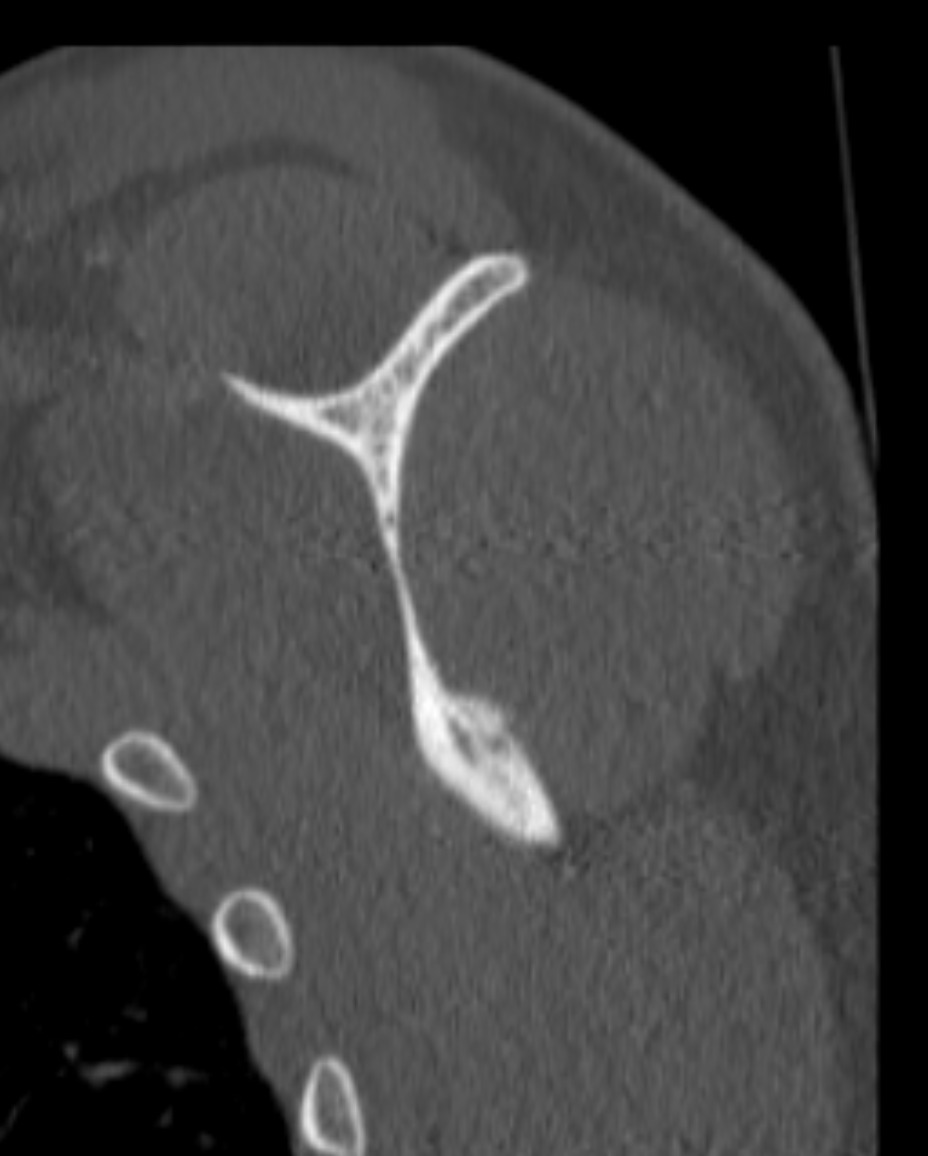
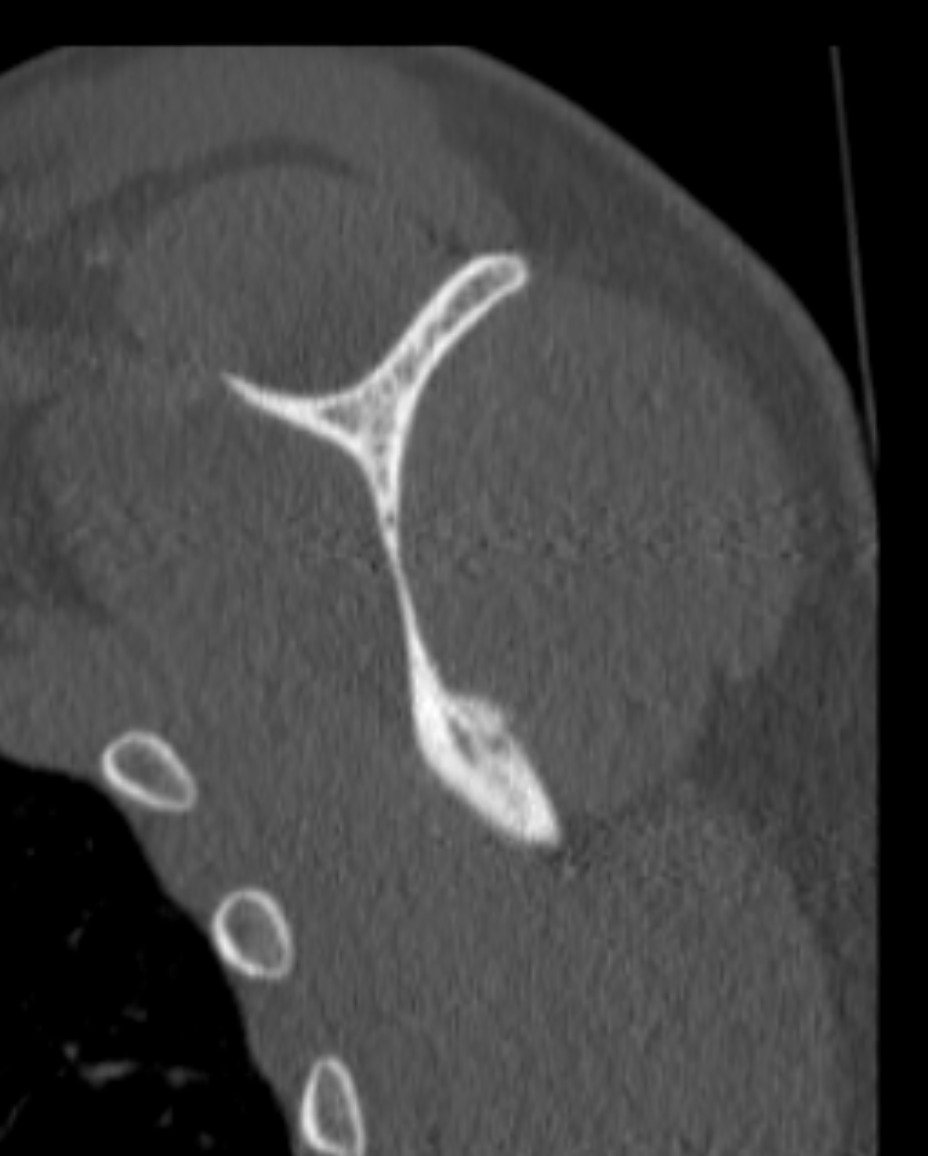
Imaging

_of_the_left_shoulder-_superior_scapular_level.png)

Imaging Results
Initial X-Ray on presentation was read and showed no obvious evidence of acute osseus abnormalities. A CT scan was ordered due to high index of suspicion. A non-displaced fracture involving the lateral scapular body was confirmed. Upon subsequent X-Ray one month later, a nondisplaced fracture was identified along the lateral margin of the infraspinous scapula, with some bony resorption along the fracture line since the previous examination. The final X-Ray two months later showed a persistent fracture line measuring approximately 1.5 milimeters. However, the fracture line was decreased with interval deposition of callus since the previous X-Ray.
Final Diagnosis
Closed non-displaced fracture of Left Scapular body
Outcomes and Return to Activity
The patient was advised to avoid overhead activities and use a sling for one week, with NSAIDs for pain management. At two-week follow-up, pain had improved, although discomfort persisted with certain movements. Four weeks post-injury, controlled rehabilitation was initiated, focusing on restoration of shoulder mobility. At two months, X-rays demonstrated routine healing, and the patient was cleared to resume upper-body strengthening and sports participation as tolerated. By the final follow-up at three months post-injury, he completed physical therapy, resumed cricket competition, and reported complete resolution of symptoms without any functional limitation.
DISCUSSION
Scapular fractures are rare (< 1% of all fractures)- usually caused by trauma, such as direct blows or falls.1 In cricket, shoulder girdle injuries are often related to bowling or fielding, but direct impact can also cause scapular body fractures.2 These injuries may initially be overlooked on X-ray due to overlying structures and subtle cortical changes. Advanced imaging is important when clinical suspicion is high. In this case, the history and exam were suspicious, even though the initial X-Ray report did not identify a fracture. The combination of localized tenderness and mechanism of injury prompted CT evaluation, which confirmed the non-displaced fracture.
Shoulder injuries in cricket are most common with bowling and throwing mechanics due to repetitive overhead motion and high eccentric loads and stress placed on the rotator cuff and labral structures.3 However, fielding-related injuries represent an important yet underreported mechanism, particularly when athletes dive or fall directly onto the shoulder. Direct axial loading to the shoulder girdle during such events can result in infrequent injuries such as scapular body fractures.3 These injuries may be initially overlooked on radiographs due to overlapping anatomical structures, but this underscores the significance of correlating imaging findings with clinical presentation and the mechanism of injury. The diagnosis and treatment of scapular fractures vary and depend on fracture location, displacement, and involvement of surrounding structures. Initial evaluation relies on advanced imaging, as many fractures, particularly that of the scapular body, are best characterized with CT scan.4 In general, fractures of the glenoid neck, coracoid, acromion, or superior shoulder suspensory complex structures warrant careful assessment when displaced, due to their potential to compromise shoulder girdle mechanics.4 In contrast many scapula fractures are minimally displaced, due to the highly vascular muscular envelope of the scapula.4 These fractures therefore demonstrate better outcomes with non-operative management. In our case, identifying the fracture line on the scapular body aided in diagnosis, and warranted a treatment similar to other extra-articular fractures, including activity modification, analgesia, and guided range of motion exercises.4