INTRODUCTION
Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of preventable morbidity and mortality in the United States.1 This review paper provides a comprehensive summary of contemporary dyslipidemia management, emphasizing advanced risk markers and imaging in primary care. While LDL cholesterol reduction is the cornerstone of prevention,2 contemporary practice increasingly incorporates advanced lipid markers, novel pharmacotherapies, and coronary imaging tools to better identify high-risk patients and personalize treatment strategies. Family physicians play a central role in early detection and management. This review summarizes modern approaches to dyslipidemia treatment, evaluation of statin intolerance,3 use of non-statin therapies,2 and the expanding role of lipoprotein(a) [Lp(a)], apolipoprotein B (ApoB), coronary artery calcium (CAC) scoring,4,5 and coronary CT angiography (CTA) in clinical decision-making.6,7
FOUNDATIONS OF DYSLIPIDEMIA MANAGEMENT IN PRIMARY CARE
Lifestyle modification remains the foundation of ASCVD prevention and is essential regardless of pharmacotherapy.1 Core strategies include weight reduction, increased aerobic and resistance activity, smoking cessation, limiting alcohol, and reducing animal-derived saturated fats. Even modest changes can meaningfully reduce ApoB-containing particles and cardiovascular risk.8 Medication management should supplement not replace behavioral interventions.
Non-adherence remains a major barrier to disease treatment, these are influenced by age, sex, ethnicity, health literacy and provider communication.9 Solutions are multidisciplinary teams, digital reminders, improved provider education, and patient centered communication strategies. Additionally, barriers to novel lipid lowering therapies include cost, regulatory hurdles, and disparities in healthcare infrastructure.10,11
STATINS: FIRST-LINE THERAPY AND PRACTICAL APPROACHES
Statins remain the most effective, evidence-based therapy for LDL reduction and event prevention. Moderate- to high-intensity statins should be initiated in high-risk patients and titrated to the maximally tolerated dose to achieve LDL goals, ideally <55 mg/dL in very high-risk individuals.2
True statin intolerance is uncommon. Best practices include discontinuing the statin until symptoms resolve, then rechallenging with a different statin at the lowest FDA-approved dose.3 Hydrophilic statins (rosuvastatin, pravastatin) are preferred due to lower CYP3A4 metabolism. If symptoms persist, intermittent dosing with long half-life statins may be considered. To qualify as true intolerance, symptoms must recur with ≥2 statins, including one at the lowest dose. Patients may exhibit partial intolerance (low-dose tolerance only) or complete intolerance (symptoms at lowest doses of ≥2 statins).12
NON-STATIN THERAPIES: EXPANDING THE TREATMENT ARMAMENTARIUM
Non-statin therapies provide important adjuncts for patients who do not achieve LDL goals with statins alone or who exhibit statin intolerance. Ezetimibe, which inhibits intestinal cholesterol absorption, offers modest LDL reduction and event benefit when combined with statins, as shown in the IMPROVE-IT trial.12 PCSK9 inhibitors are monoclonal antibodies that prevent LDL receptor degradation and can lower LDL to 20–30 mg/dL with demonstrated morbidity and mortality benefit.2 Bempedoic acid inhibits cholesterol biosynthesis upstream of HMG-CoA reductase, reducing LDL by approximately 15% with a low risk of muscle-related side effects.2 Finally, icosapent ethyl (purified EPA) lowers triglycerides and has shown event reduction in patients with elevated triglycerides despite statin therapy.2
BEYOND THE STANDARD LIPID PANEL: ADVANCED MARKERS FOR RISK STRATIFICATION
Lipoprotein(a) [Lp(a)] is genetically determined and a strong independent risk factor for CAD, MI, stroke, and aortic stenosis.13,14 Testing is recommended once in adulthood, particularly for those with family history or unexplained premature CAD. PCSK9 inhibitors offer modest reductions; emerging agents such as pelacarsen and olpasiran reduce Lp(a) by 80–90% in trials but are not yet FDA-approved.15,16
Apolipoprotein B [ApoB] reflects the number of atherogenic particles and is a superior predictor of risk in diabetes, metabolic syndrome, and hypertriglyceridemia.17 ACC/AHA guidelines consider ApoB >130 mg/dL a risk enhancer, with a goal of <80–90 mg/dL in high-risk patients.2
CORONARY IMAGING IN PREVENTION AND DIAGNOSIS
Coronary Artery Calcium (CAC) scoring is a non-contrast CT used for primary prevention in asymptomatic adults aged 40–75 years when statin decisions are uncertain.4,5 CAC = 0: Very low short-term risk; reasonable to defer statin therapy. CAC 1–99: Statin favored, especially age >55. CAC ≥100: Statins strongly recommended; CAC ≥400 indicates very high risk.4,5 Not appropriate for chest pain evaluation or patients with diabetes or LDL >190 mg/dL (already statin-indicated).1
Coronary CT Angiography (CTA) is a contrast-enhanced CT for evaluating symptomatic patients with suspected CAD. Best for stable chest pain and intermediate pre-test probability. Benefits include identification of stenosis and plaque morphology, a long ‘warranty period’ after a negative CTA, and detection of non-obstructive plaque prompting preventive therapy. Key distinction: CAC is a screening tool for asymptomatic individuals; CTA is diagnostic for symptomatic patients.6,7
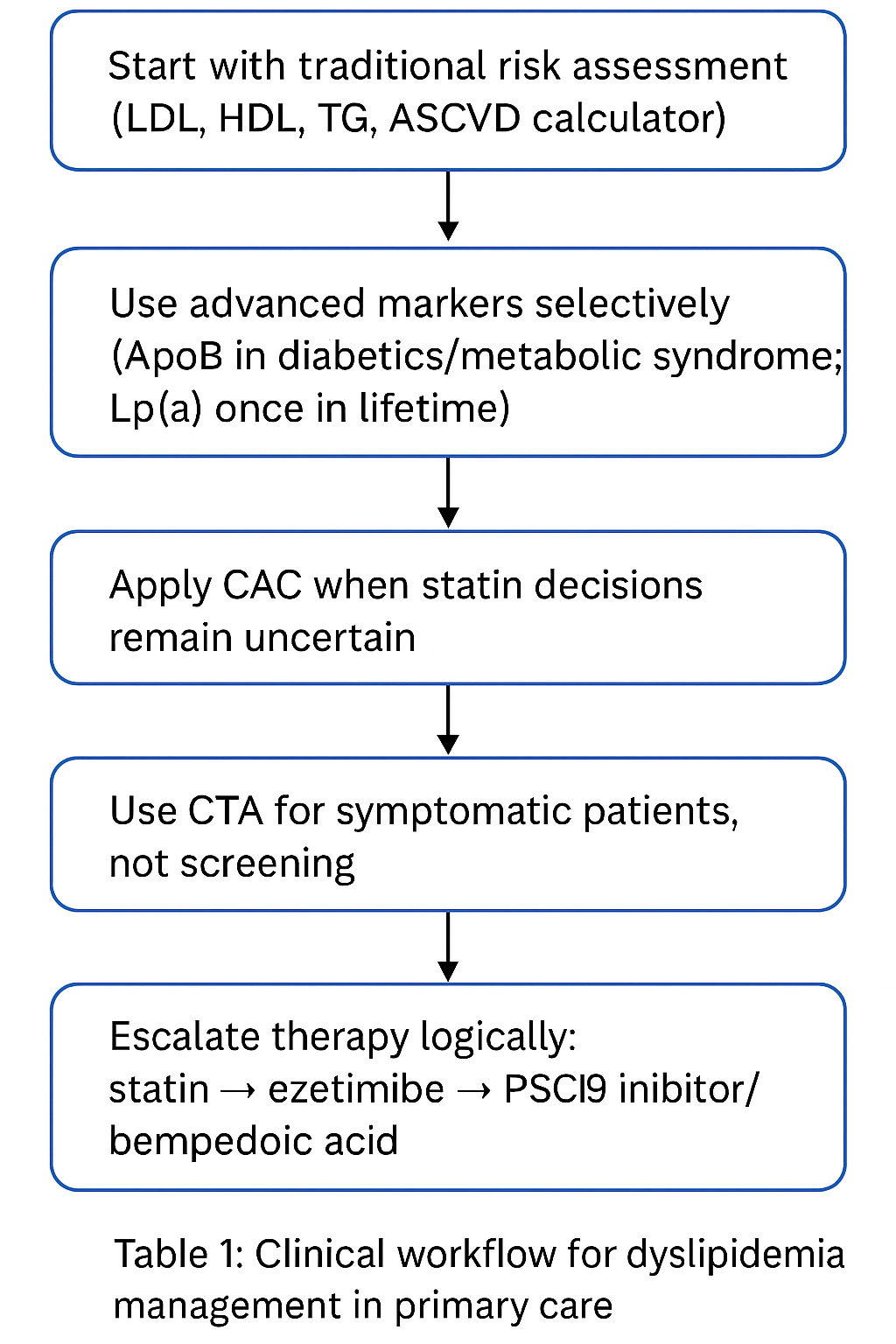
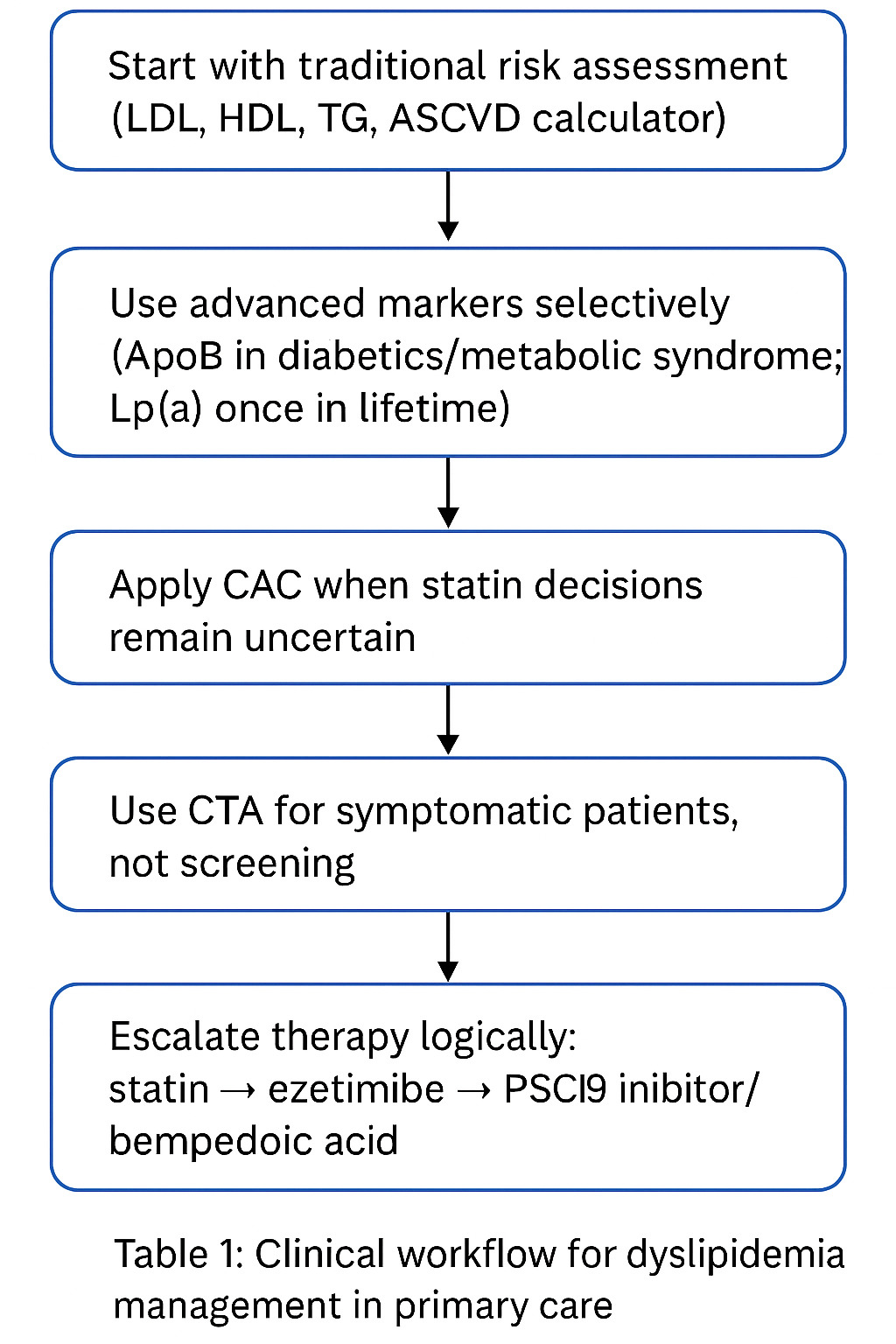
CLINICAL INTEGRATION FOR THE PRIMARY CARE PHYSICIAN
A practical workflow is described below in table 1: Start with traditional risk assessment (LDL, HDL, TG, ASCVD calculator). Use advanced markers selectively (ApoB in diabetics/metabolic syndrome; Lp(a) once in lifetime). Apply CAC when statin decisions remain uncertain. Use CTA for symptomatic patients, not screening. Escalate therapy logically: statin → ezetimibe → PCSK9 inhibitor/bempedoic acid. Treat to appropriate intensity, not just numbers.
CONCLUSION
Modern dyslipidemia management extends beyond the traditional lipid panel. Incorporating advanced markers such as Lp(a) and ApoB, alongside imaging modalities like CAC scoring and CTA, enables clinicians to more accurately identify patients at risk for premature cardiovascular disease. Statins remain first-line therapy, but non-statin options—including ezetimibe, PCSK9 inhibitors, bempedoic acid, and icosapent ethyl—provide effective adjuncts. For family physicians, combining pharmacologic therapy with advanced screening tools allows for precise, individualized cardiovascular prevention and improved long-term outcomes.1