
INTRODUCTION
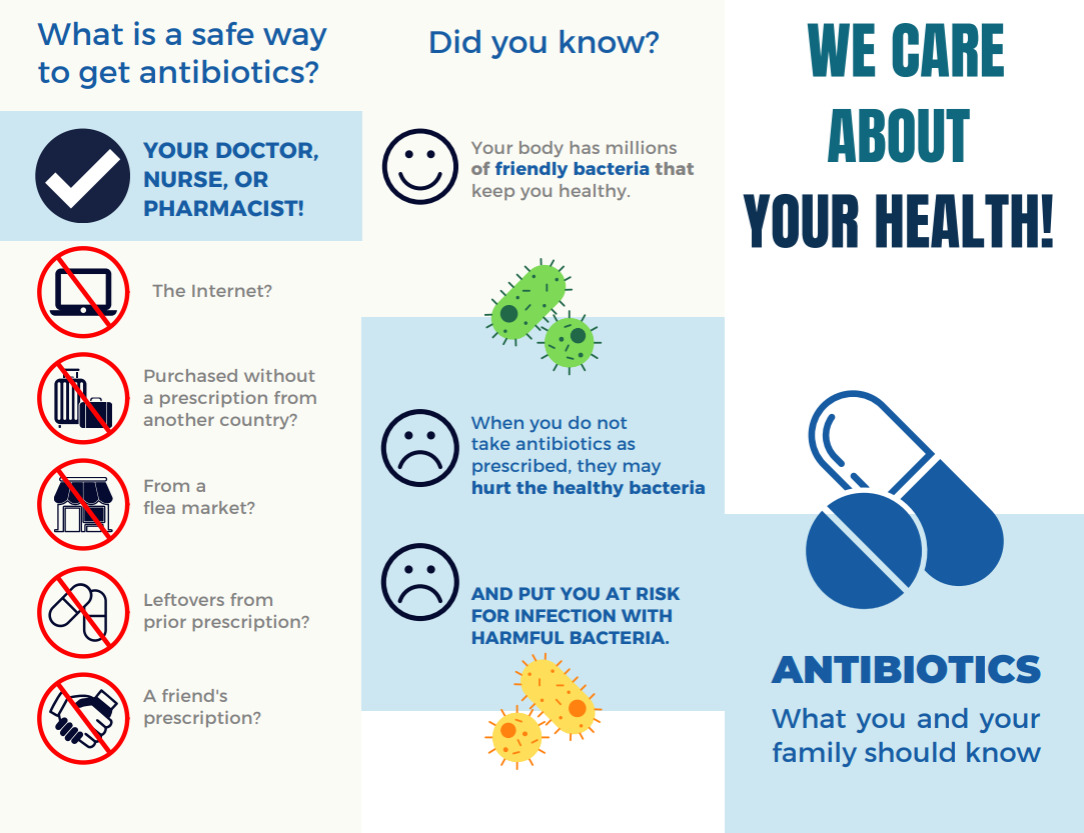
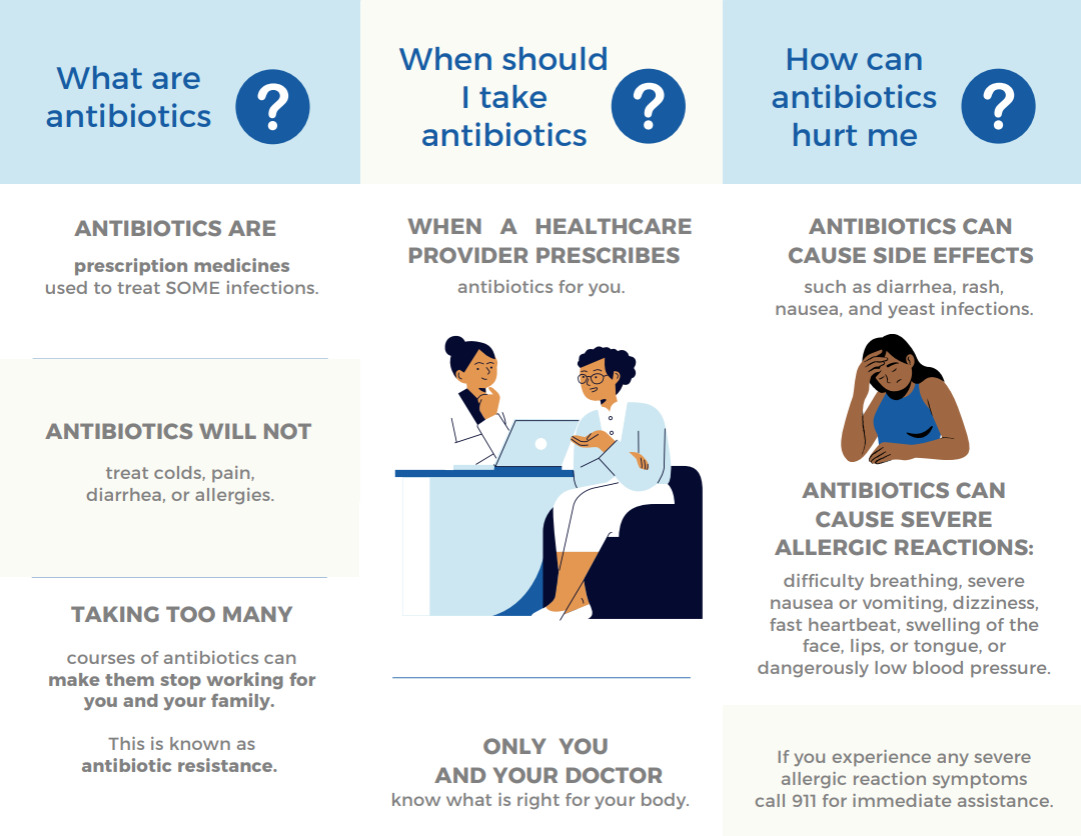
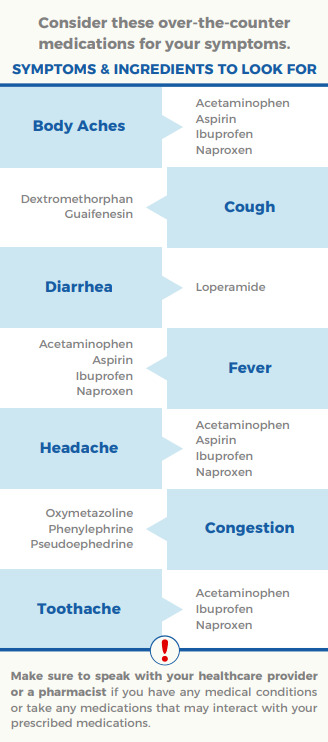
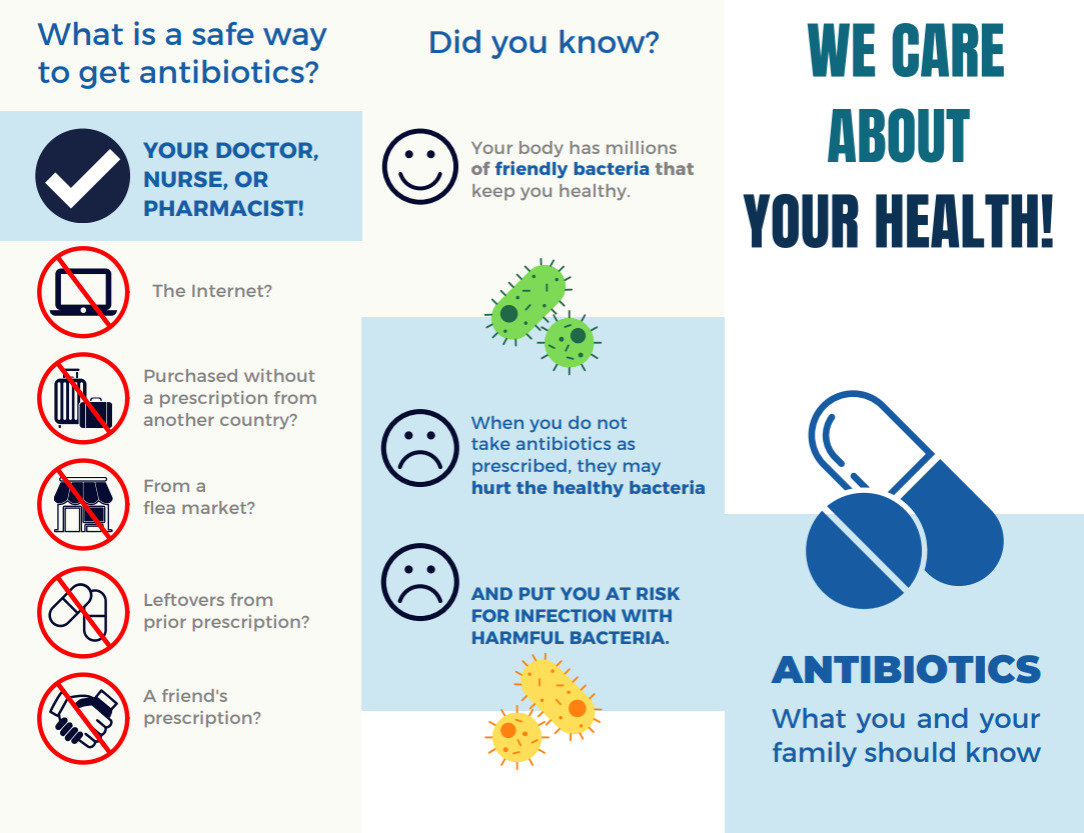
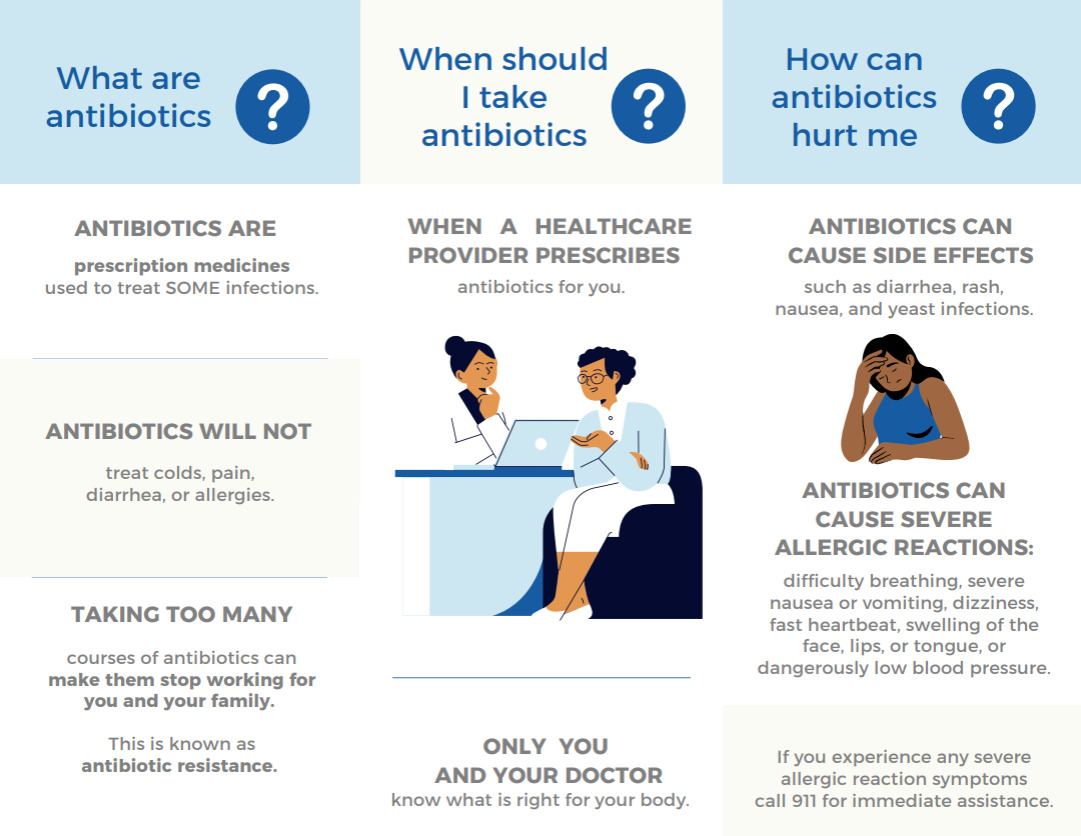
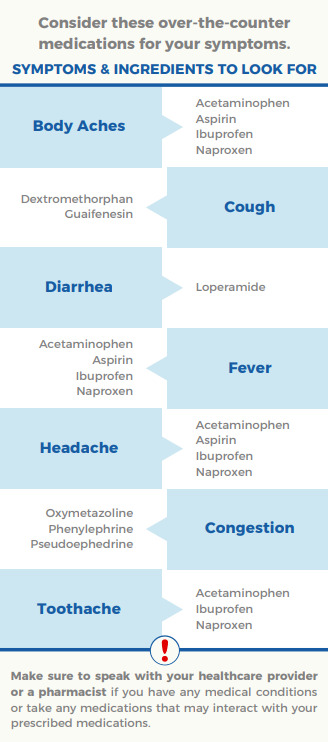
Use of antibiotics without a prescription (non-prescription use) is common in the United States (US) and presents an important safety issue.1 At the public health level, non-prescription use leads to inappropriate antibiotic use, thereby increasing the risk of antimicrobial resistance.2 At the individual level, safety issues related to non-prescription use include adverse drug reactions, drug interactions, masking underlying infectious processes, superinfection, and disruption of the healthy microbiome.3 Sources of antibiotics used without a prescription or stored for future use include stores, yerberias (i.e., herbalist shops) or flea markets, “leftover” antibiotics from previous prescription, or antibiotics obtained abroad, on-line or from a relative or friend.4–6 Recent US surveys showed that the prevalence of non-prescription antibiotic use varied from 20% to 45%.7 In a 2023 survey of primary care patients in Texas, 43.8% reported using nonprescription antibiotics, and 31.4% expressed intention to use antibiotics without a prescription.8 To reduce this unsafe practice, we developed an educational brochure, “Antibiotics: what you and your family should know” (Appendix A). Our brochure is informed by the findings of previous qualitative and quantitative studies exploring the factors contributing to non-prescription use.8,9 For example, we found that many patients expect antibiotics in an attempt to relieve acute diarrhea and certain symptoms from viral infections (i.e., influenza).10 Therefore, our tool emphasizes that antibiotics will not treat these symptoms and provides a list of over-the-counter medications to alleviate them. We used an iterative design with feedback from six racially and ethnically diverse community advisory board members, family medicine clinicians and a graphic designer. In addition, two experts in health literacy and cultural and linguistic competency in Hispanic communities provided their input. The brochure (English and Spanish versions) included information on safe means of obtaining antibiotics, antibiotic side effects, non-antibiotic treatment of common symptoms with over-the-counter alternatives, and how to access care at publicly funded clinics.
In this study, we surveyed family medicine patients to evaluate our brochure’s acceptability, appropriateness, and usability in educating patients about safe antibiotic use and the risks of non-prescription use.
METHODS
The patient surveys were conducted in English and Spanish, and were performed in two private, academically affiliated family medicine clinics in a large urban area. Both clinics provide acute and preventative care, behavioral health, and nutrition services to insured and uninsured patients.
Patient Recruitment and Selection
Eligible participants were adult patients (≥18 years) residing in Harris County or Katy who were able to communicate in English or Spanish. Patients were excluded if they were <18 years of age or unable or unwilling to complete the survey. Participants were recruited at participating clinical sites during the study period using a consecutive sampling of eligible patients, with enrollment monitored and guided to achieve prespecified race and ethnicity representation. Those who provided informed consent were enrolled in the study.
Patients who agreed to participate reviewed the brochure in their preferred language (English or Spanish) and completed the survey that was read aloud by bilingual research coordinators. The response rate for the survey was 92%. Participants were reimbursed $20 for their participation. This project was approved by the IRB at Baylor College of Medicine and Harris Health (H-45709).
Patients completed a survey about the brochure’s acceptability, appropriateness, and usability followed by an open-ended question about suggested improvements (Appendix B). Acceptability was defined as the patients’ perception that the brochure is acceptable and included the following questions, “the brochure meets my approval,” “the brochure is appealing to me,” “I like the brochure,” and “I welcome the brochure.”11 Appropriateness was defined as patients’ perception of the fit and relevance of the brochure to the local context.11 For acceptability and appropriateness, the responses were rated on a 5-point Likert scale ranging from “completely disagree to completely agree” Usability questions were included to assess readability, comprehensibility and usefulness of the brochure, and were similarly rated on a 5-point Likert scale (Appendix B).12 Survey participants who answered “not useful” to any usability questions were asked to share their thoughts on ways to improve the brochure’s usefulness. Participants were also asked demographic questions (i.e. education level, sex, race/ethnicity, etc.) and questions to evaluate health literacy using the Brief Health Literacy Screen measure.13,14
Sample size calculation
Our target for each of these primary outcomes was at least 80%, because we felt 80% was a good threshold to target among potential end-users of this brochure. For example, the brochure was considered acceptable if at least 80% of surveyed patients indicated they “completely agree” or “agree” using the validated acceptability measure. Based on an expected prevalence of 80% and a precision of 8%, a sample size of 97 was calculated. Therefore, we recruited 100 patients (50 from each clinic) to complete the survey.
Statistical analysis
Descriptive statistics were performed on all variables. For each outcome, the mean and standard deviation were calculated. We also reported the proportion of patients who thought the tool was acceptable, appropriate, and/or useful. We categorized open-ended answers from patients on why they did or did not find the brochure useful.
RESULTS
Survey participants (N = 100) had a mean age of 53 years, 72% female, 72% college educated, and 81% adequate health literacy (Table 1). Our sample was primarily composed of Black or African American (35%), Hispanic or Latino (35%), and Non-Hispanic White (28%) participants. The survey achieved a high response rate of 92%.
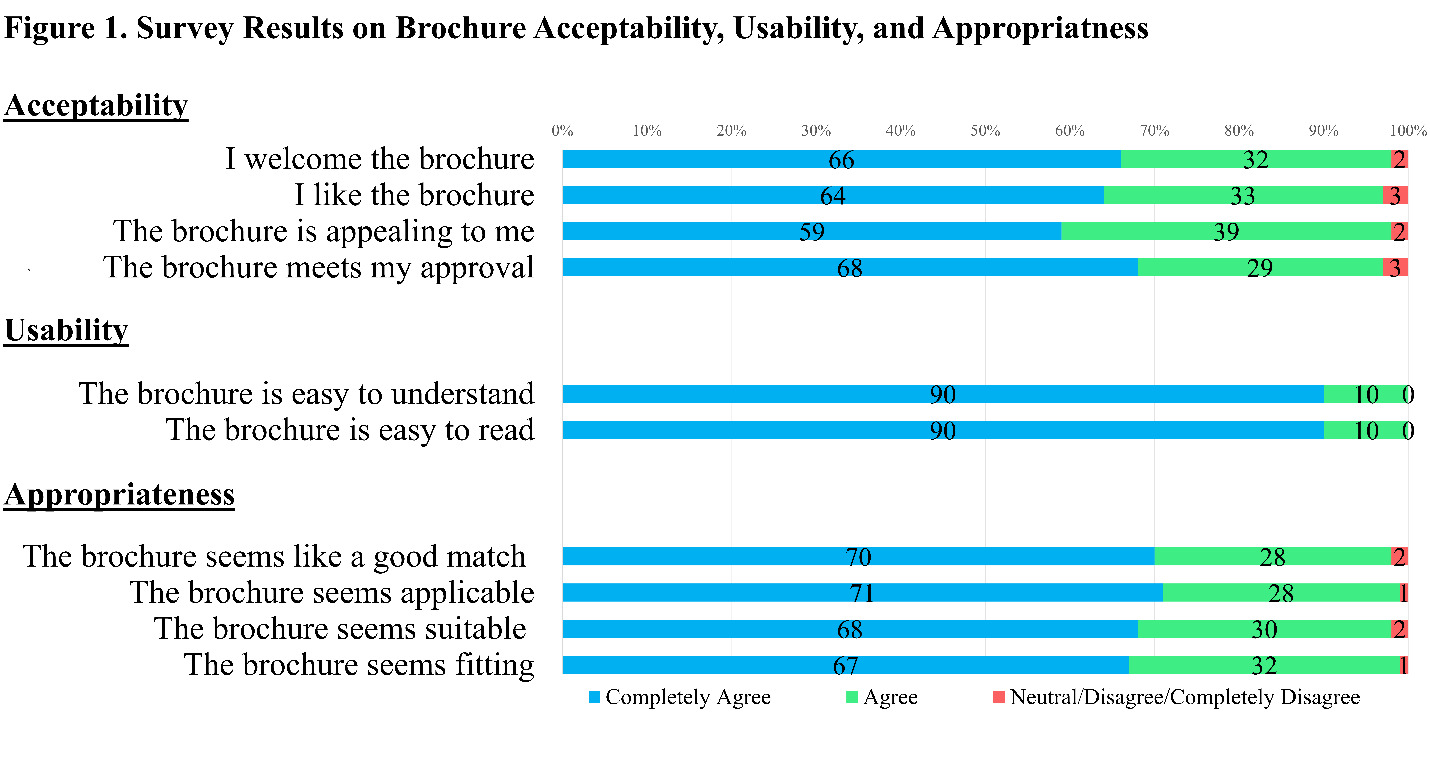
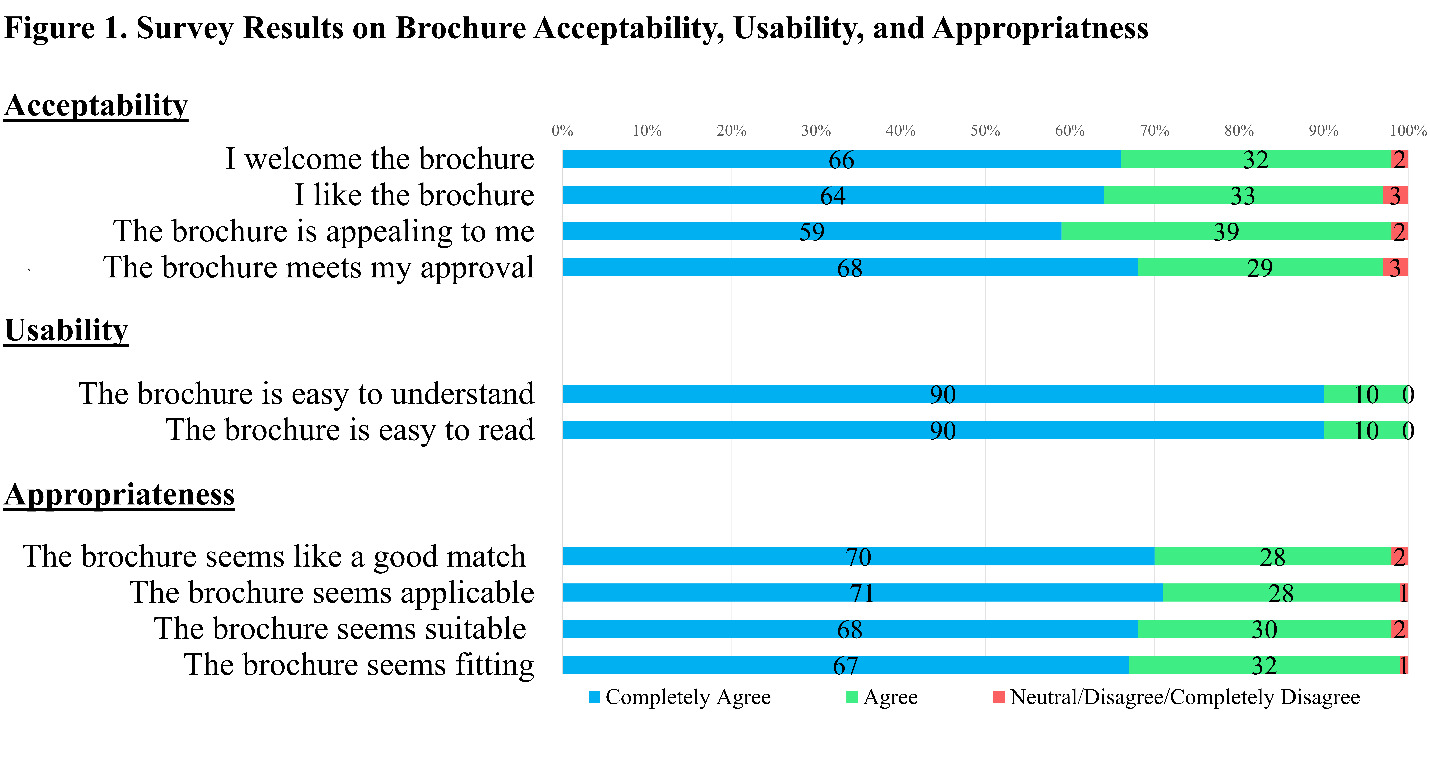
The brochure was deemed acceptable (98%), usable (100%), and appropriate (98%) (Figure 1). Expanding on the results, the majority of participants rated the brochure positively: 98% welcomed it, 97% liked it, and 98% found it appealing. Regarding the usability of the brochure. Participants found the brochure easy to read (100%), and 97% approved of it. In terms of appropriateness, 99% found it applicable, 98% considered it a good match for most patients, 98% rated it as suitable, and 99% as fitting. The most cited reasons participants found the brochure useful included learning new information about antibiotic indications (23%), with one participant stating, “[The brochure] Explain[s] a lot. Didn’t know about information about antibiotics,” and another remarking, “[I] learned that antibiotics do not treat cold and allergies.” Over-the-counter alternatives for symptom relief were also frequently mentioned (23%) as a positive attribute of the brochure with comments such as, “[The brochure] provided a lot of information with regards to alternatives to antibiotics.” Additionally, 14% highlighted learning about antibiotic side effects, exemplified by the quote, “[I] didn’t know antibiotics have side effects.” Participants also stated that the brochure was readily comprehensible and culturally appropriate, illustrated by participants remarks such as “[The brochure] is simple, easy to read, [and the] language is easy to understand” and “It explains [a] lot of things in layman terms, very appealing. [The] visuals are nice. [The brochure] is very specific for [the] culture.”
The most common reason (4%) for finding the brochure not useful was that the participants “knew everything in the brochure.” The most common suggestions for improvement included to provide alternative media such as audio format and having it available at pharmacies (each suggested by 4 participants).
DISCUSSION
Our educational brochure was well received by a sample of adults with diverse racial and ethnic backgrounds. The high levels of acceptability (98%), usability (100%), and appropriateness (98%) reported by participants suggest that the brochure’s design and content were effectively tailored to the target population. Participants also reported perceived improvements in understanding of antibiotic indications (23%), the availability of over-the-counter alternatives for symptom relief (23%), and the potential for antibiotic side effects (14%). Overall, these findings suggest that well-designed patient-facing educational materials are an acceptable tool that may help address gaps in antibiotic knowledge in community settings.
By addressing knowledge gaps, our brochure may help mitigate patient-driven factors associated with non-prescription antibiotic use. Prior work has largely focused on inappropriate prescribing within clinical encounters. Although leaflet and brochure-based interventions have been previously evaluated, these efforts have primarily been implemented within clinical settings with focus on prescribing behaviors. These approaches have less often directly targeted patient-driven non-prescription antibiotic use or incorporated community stakeholder input. In contrast, this pilot study evaluates the acceptability of a culturally tailored, patient education tool designed for community-engaged settings, including its potential relevance to non-prescription antibiotic use. However, direct evidence linking leaflets or brochure-based educational materials to reductions in non-prescription antibiotic use remains limited.
Inappropriate antibiotic use and non-prescription antibiotic use appear to share overlapping drivers, including misconceptions about effectiveness, treatment expectations, and retention of leftover antibiotics. We therefore hypothesize that interventions effective in reducing inappropriate use, particularly patient-facing educational materials, may also influence non-prescription use by targeting shared behavioral determinants. This interpretation is supported by prior evidence on educational interventions affecting antibiotic-related attitudes and prescribing. For example, Ritchie et al. showed that simple educational material, presented as a poster, reduced expectations for antibiotic prescriptions from 27% to 13%, particularly when emphasizing the risks and harms of antibiotic use.15 Similarly, a patient education intervention in which participants received materials on appropriate antibiotic use reduced antibiotic prescribing rates for acute bronchitis in adults from 60% to 36%.16 Although this study included an ongoing physician quality improvement component, the addition of patient-directed education produced a substantially greater reduction in prescribing than physician-focused intervention alone.16 These findings suggest that patient-facing educational strategies may have utility in antimicrobial stewardship at the community level, although their effect on non-prescription antibiotic use remains untested directly. This is particularly relevant given the limited availability of stewardship programs at the community level.17
At the patient level, beliefs and prior experiences shape expectations for antibiotics, particularly regarding perceived necessity.8 Educational interventions that are culturally appropriate and accessible may therefore represent a feasible approach to improving antibiotic-related knowledge and attitudes.
Our findings support the acceptability of a patient-facing educational brochure in primary care settings. However, several limitations should be considered. This study was conducted at two primary care clinics in Houston, TX, with a small sample size, which may limit generalizability despite consecutive stratified recruitment by race and ethnicity. As with any survey-based study, self-selection bias cannot be ruled out. Nonetheless, the high response rate suggests that such bias is unlikely to have substantially influenced the primary conclusions.
Second, we did not measure objective changes in knowledge or behavior, relying instead on participants’ self-reported perceptions after exposure to the brochure. Third, responses may have been influenced by social desirability bias, and the Hawthorne effect. Additionally, most participants (81%) demonstrated adequate health literacy, limiting assessment of differential effects across literacy levels.
This pilot study was designed to assess acceptability, appropriateness, and usability among potential end-users. Future work should evaluate performance across broader literacy strata and in more diverse populations. Importantly, knowledge change alone may be insufficient to modify non-prescription antibiotic use, which is also influenced by structural and socioeconomic factors, including costs, access to care, and convenience.7 Future studies should assess both knowledge and behavioral outcomes and examine effectiveness when combined with interventions addressing these broader determinants. Finally, larger studies in more diverse settings are needed to improve generalizability of these findings.
ACKNOWLEDGEMENTS
This project was funded by the Texas Academy of Family Physicians (TAFP)and by the Agency for Healthcare Research and Quality (1R01HS026901-01). The views expressed in this report are those of the authors and do not necessarily reflect the official policy or position of TAFP or the United States government. We would also like to thank Fara Abordaje, Tracy Fletcher-Davies, and Connie Dupler for their valuable assistance and support during the research project.
Corresponding author
Johanan Luna, Washington University, Division of Infectious Diseases, 4990 Children’s Place, St Louis, MO, 63110 e-mail: Johanan@wustl.edu